Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
| Complications | |
| Ticagrelor-Associated High-Degree Heart Block: A Case Report & Review of the Literature | |
| Hariom Tyagi1 | |
| Lokpriya Hospital, India1 | |
|
Background:
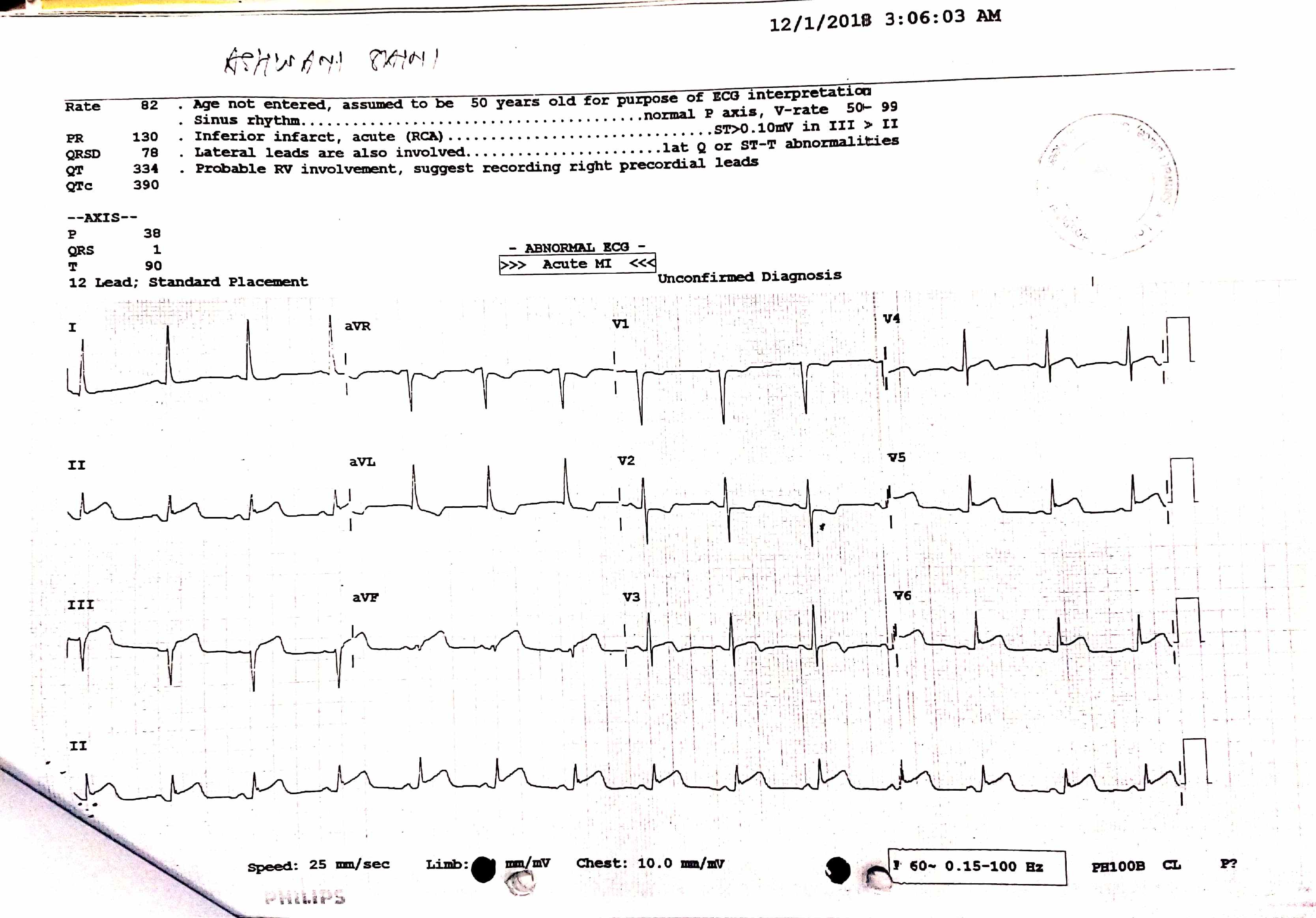
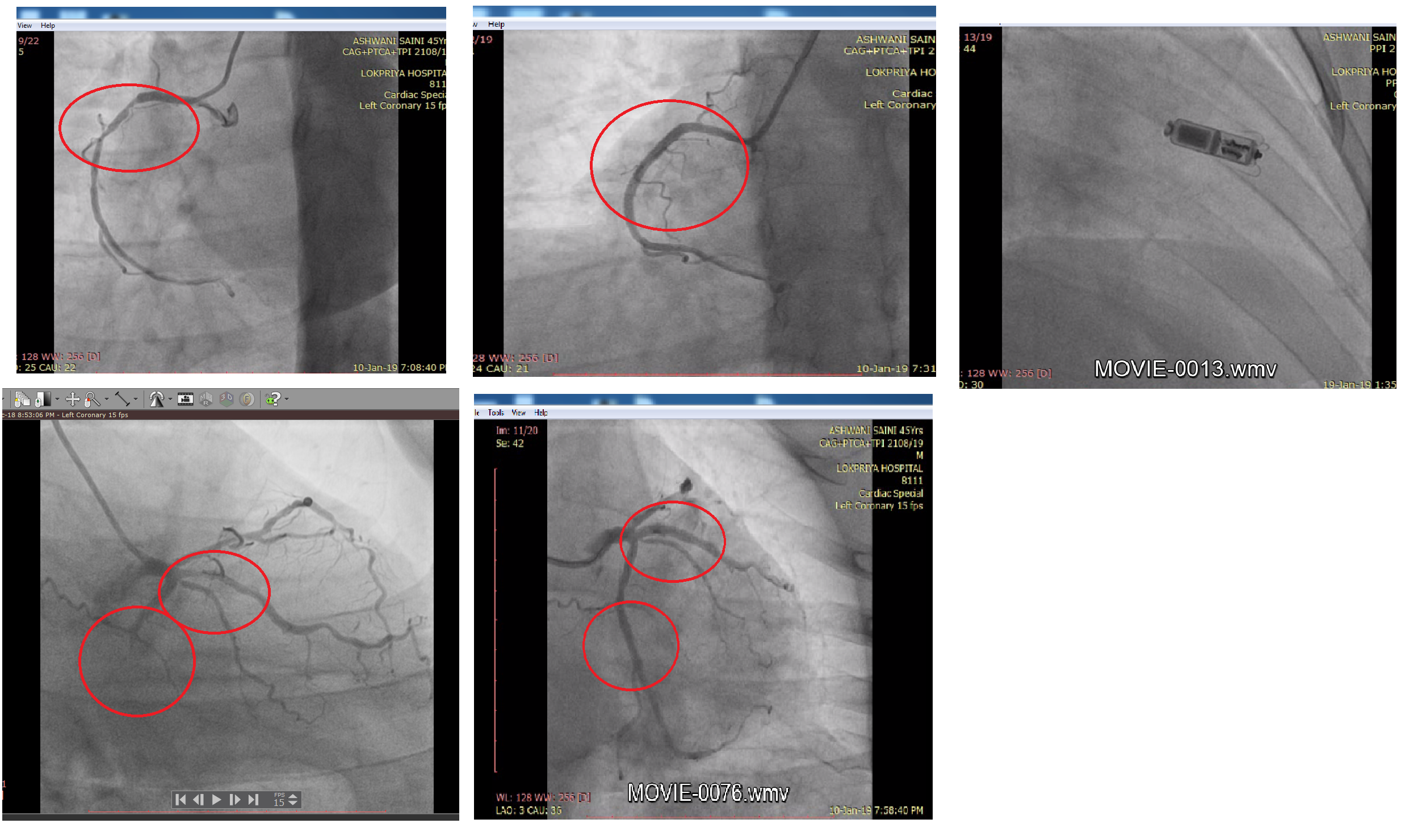
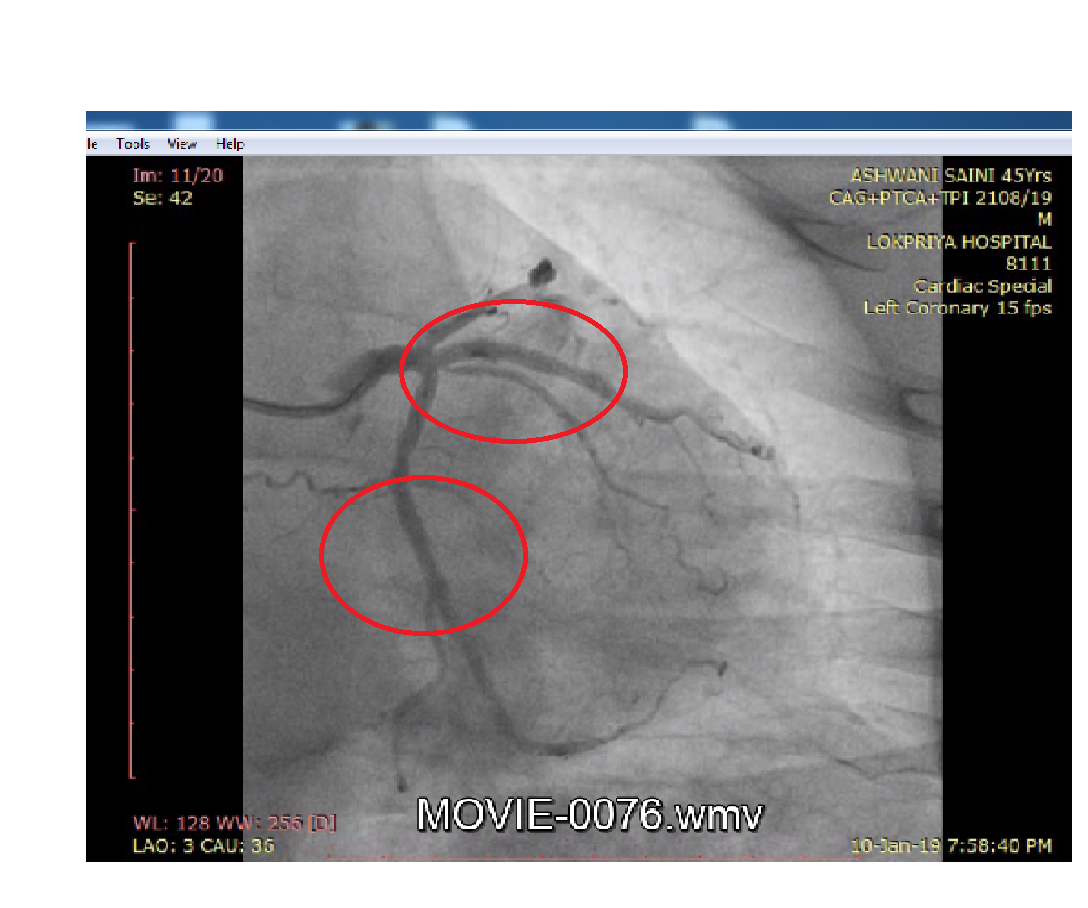
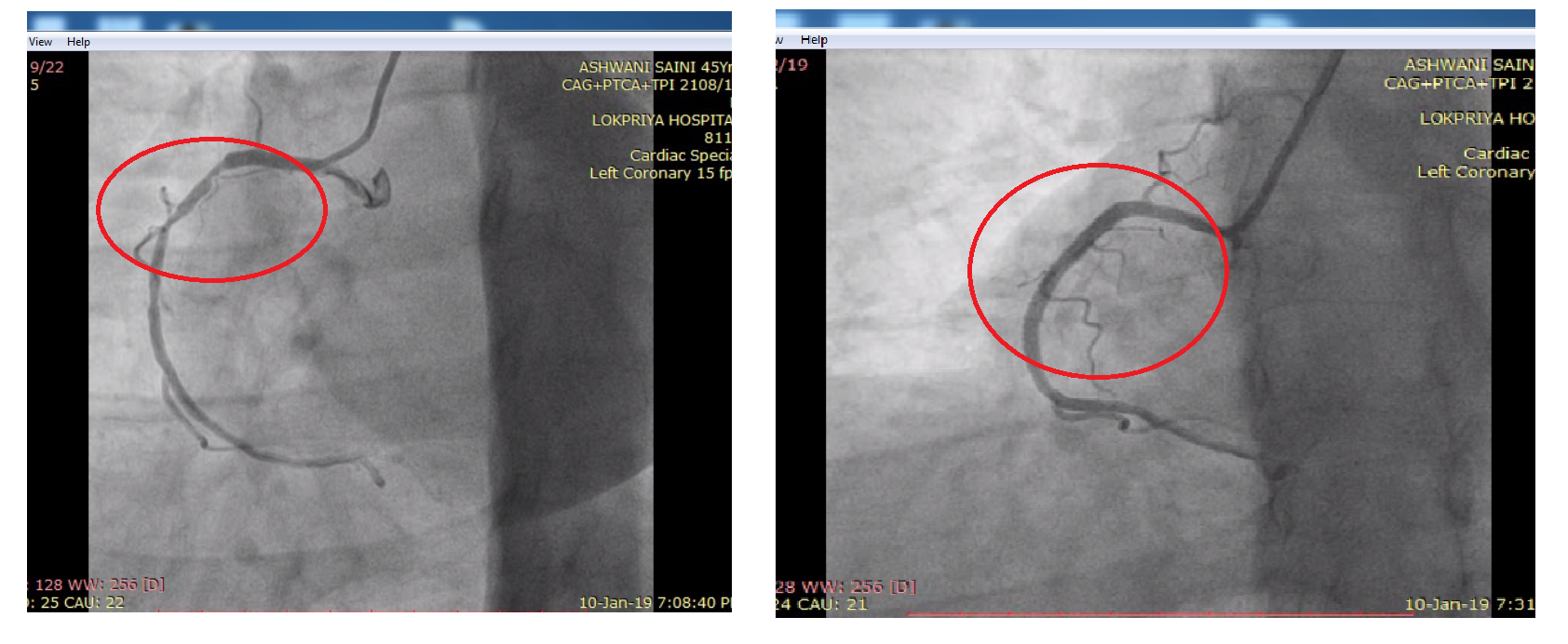
A 45-year-old male patient presented herewith H/O Pain in both upper limbs, suffocation, sweating, associated with generalized weakness for last 1 day prior to admission.ECG: ST-T elevation in inferolateral leads.ECHO: CAD/RWMA-Inferoposterior Territory Hypokinetic. Mild LV systolic dysfunction (LVEF=40-45%). Mild MR.CAG- Triple Vessel Disease: LAD: Ostio proximal to mid 60-70% disease, distal diffuse disease, D1& D2: Diseased. Ramus: Proximal 80-90% disease. LCX: Proximal 100%occlusion. OM1: Ostial 90% disease. RCA: Dominant, Proximal 90% disease, mid70-80% disease.Chest X-RAY: Bronchovascular markings are prominent.
|
|
|
Methods:
PTCA TO LCX & OM : Left Coronary Artery was engaged with EBU 3.5, 6F guide catheter. A 0.014” SION BLUE wire was used to cross the LCX& OM lesion. Pre dilatation done with SC sapphire balloon 2.0
GP IIb IIIa inhibitor was used during the procedure. Excellent result with TIMI III flow. Successful PTCA with stenting to RCA & RAMUS. 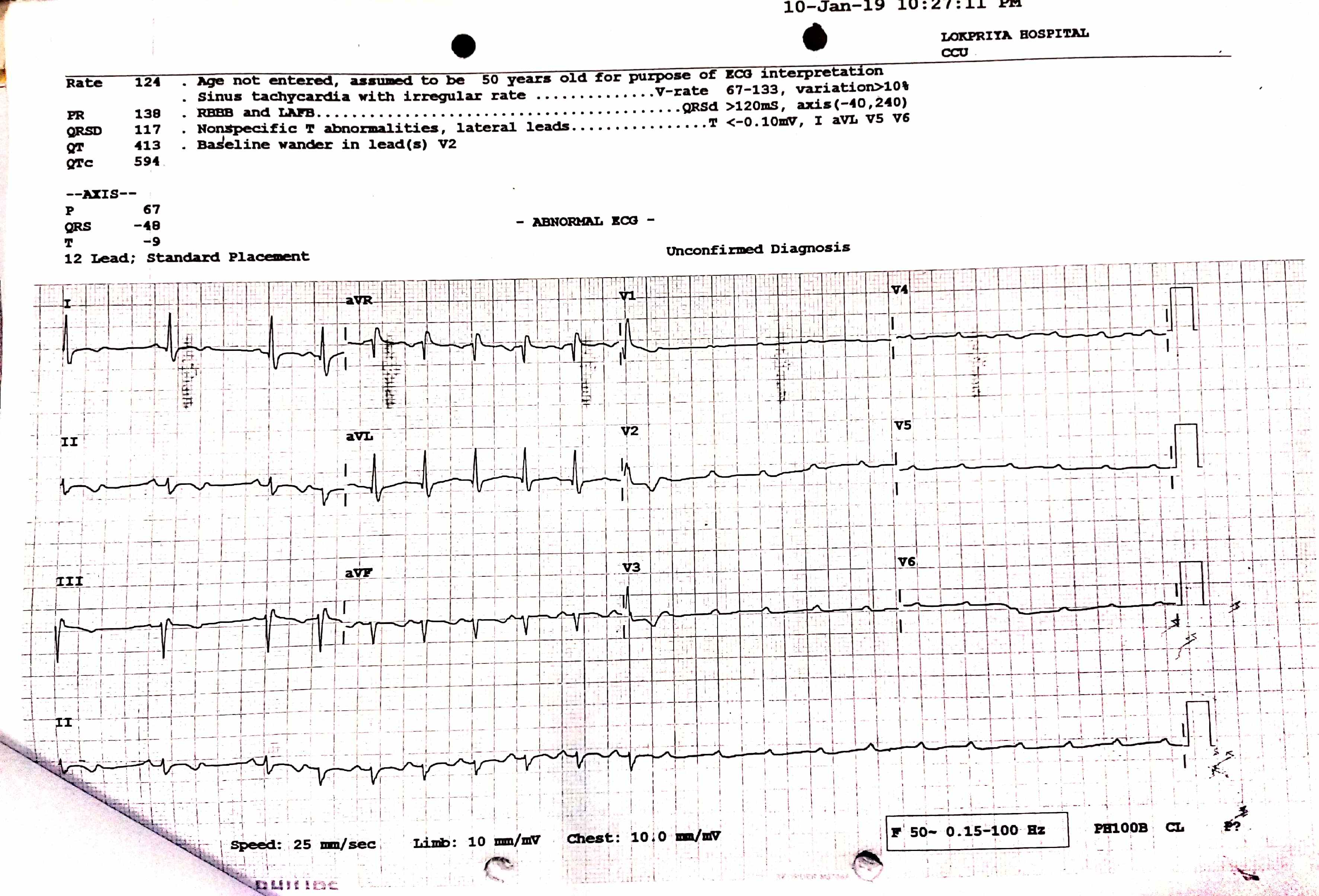 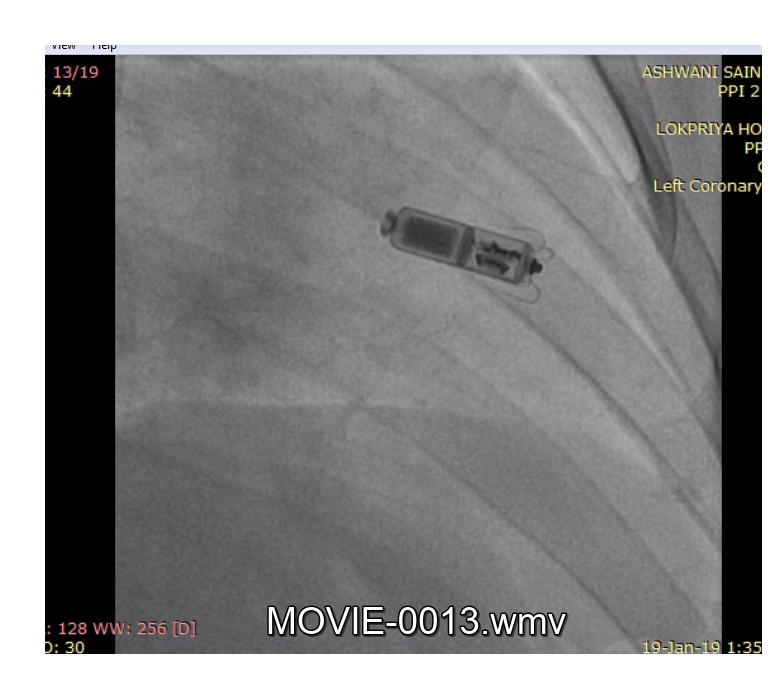 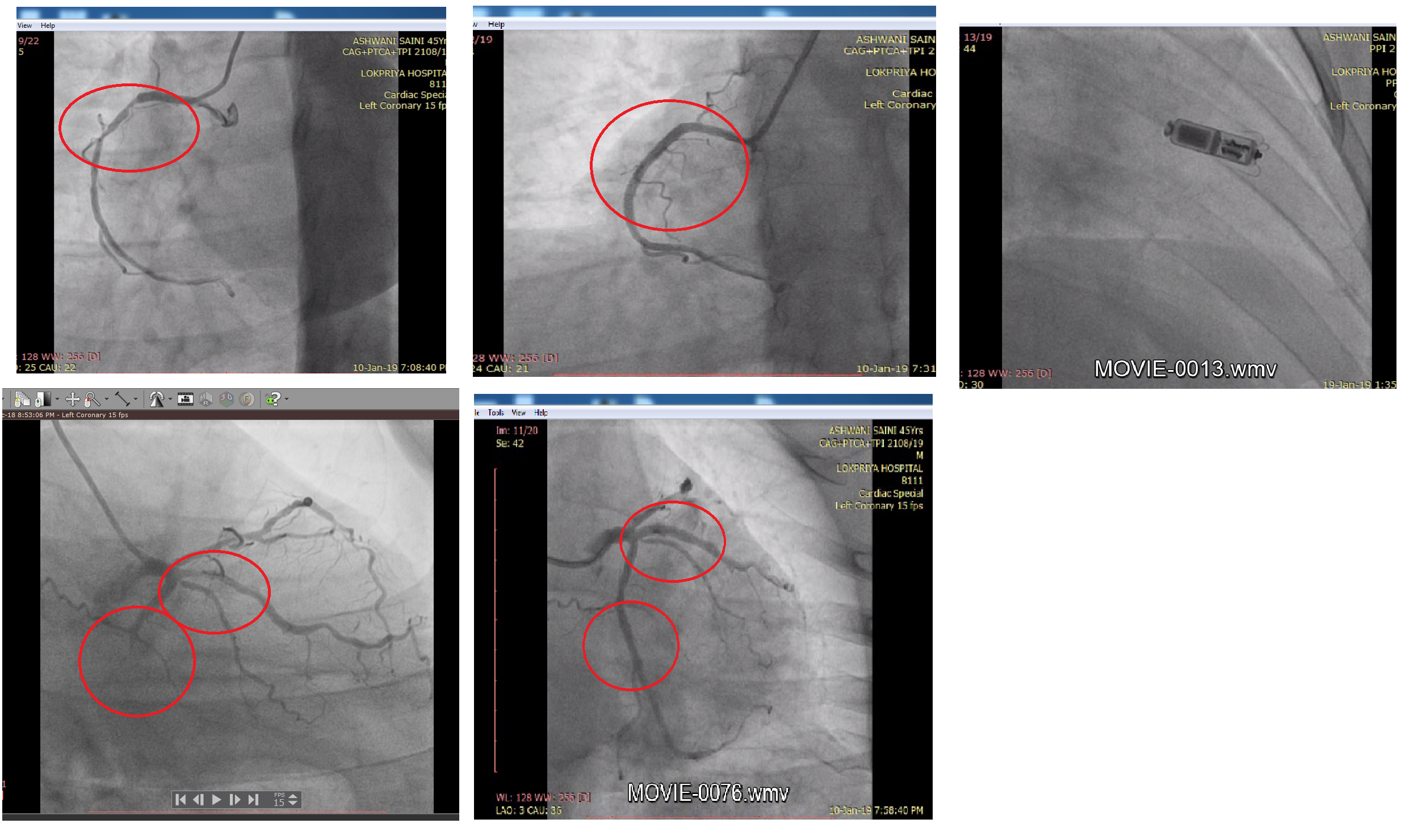 |
|
|
Results:
During hospitalization patient was taken for urgent Coronary Angiography which revealed Triple Vessel Disease and PTCATO LCX TO OM (02.12.2018)- (RESOLUTE ONYX 2.75
   |
|
|
Conclusion:
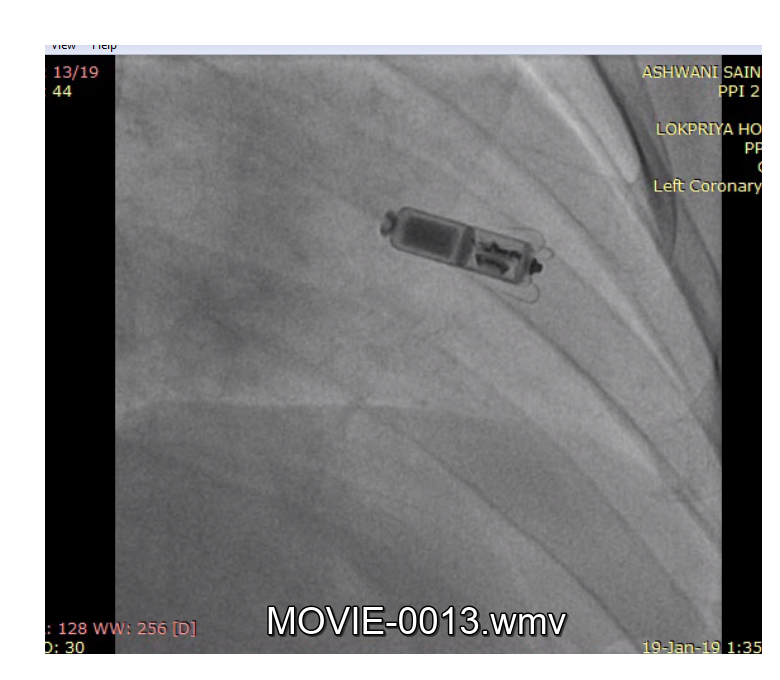
We present a case of symptomatic and profound AV node dysfunction in a patient treated with ticagrelor post-PCI for Inferior Wall MI. This was observed in our patient even in the absence of baseline conduction disease or concurrent confounding medications, unlike most cases in the published literature and highlights the need for broader awareness of ticagrelor’s not-insignificant brady-arrhythmic potential.
|
|