Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
ABS20191020_0001
| Physiologic Lesion Assessment | |
| Post Procedural Physiological Assessment of CTO Lesion | |
| Nao Yasuda1, Takuma Tsuda1 | |
| Nagoya Ekisaikai Hospital, Japan1 | |
|
Background:
Success rate of CTO-PCI have dramatically improved during decades due to development of both device and technical aspects. However physiological aspect of CTO remains unclear. This study was to assess the relationship between wire position and physiological improvement during CTO-PCI.
|
|
|
Methods:
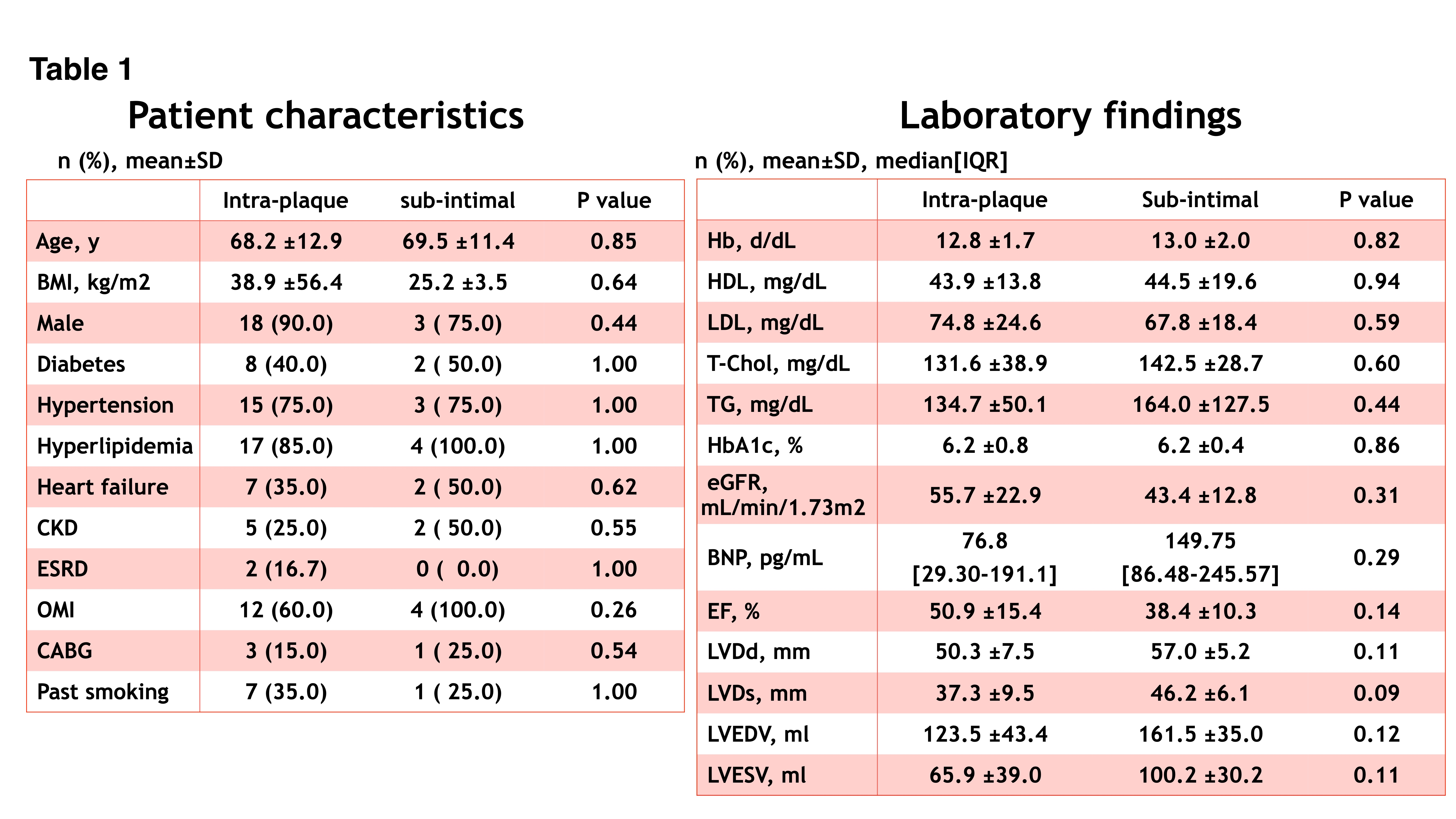
Among 2018 April to 2019 September, a total of 24 CTO cases were enrolled in this study. Resting index, FFR and pCFR were assessed after recanalizing CTO, which was compared to pre-procedural values. Moreover, we divided them into two groups regarding wire position inside CTO; All true lumen tracking was divided as true Intra-plaque group (IP group: n=20) and the other was divided as sub-intimal group (SI group: n=4) (Table1).
 |
|
|
Results:
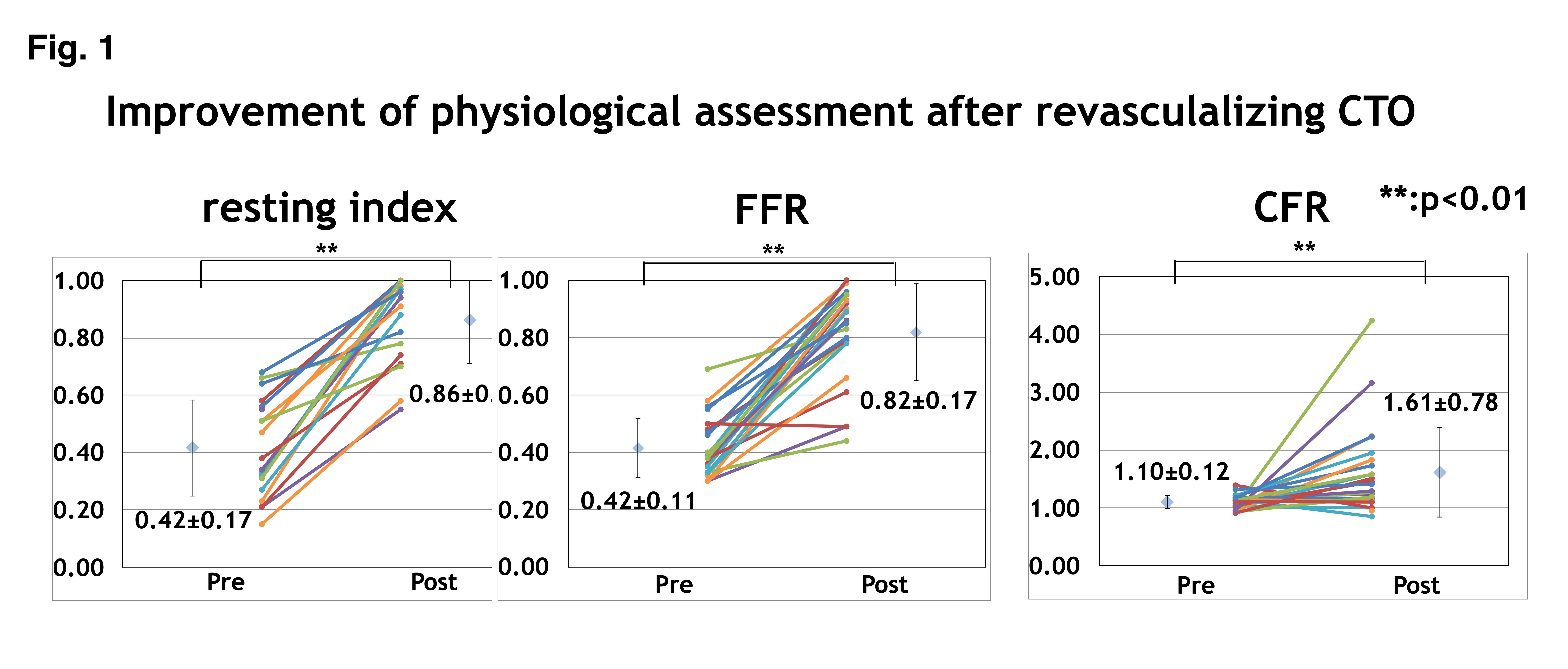
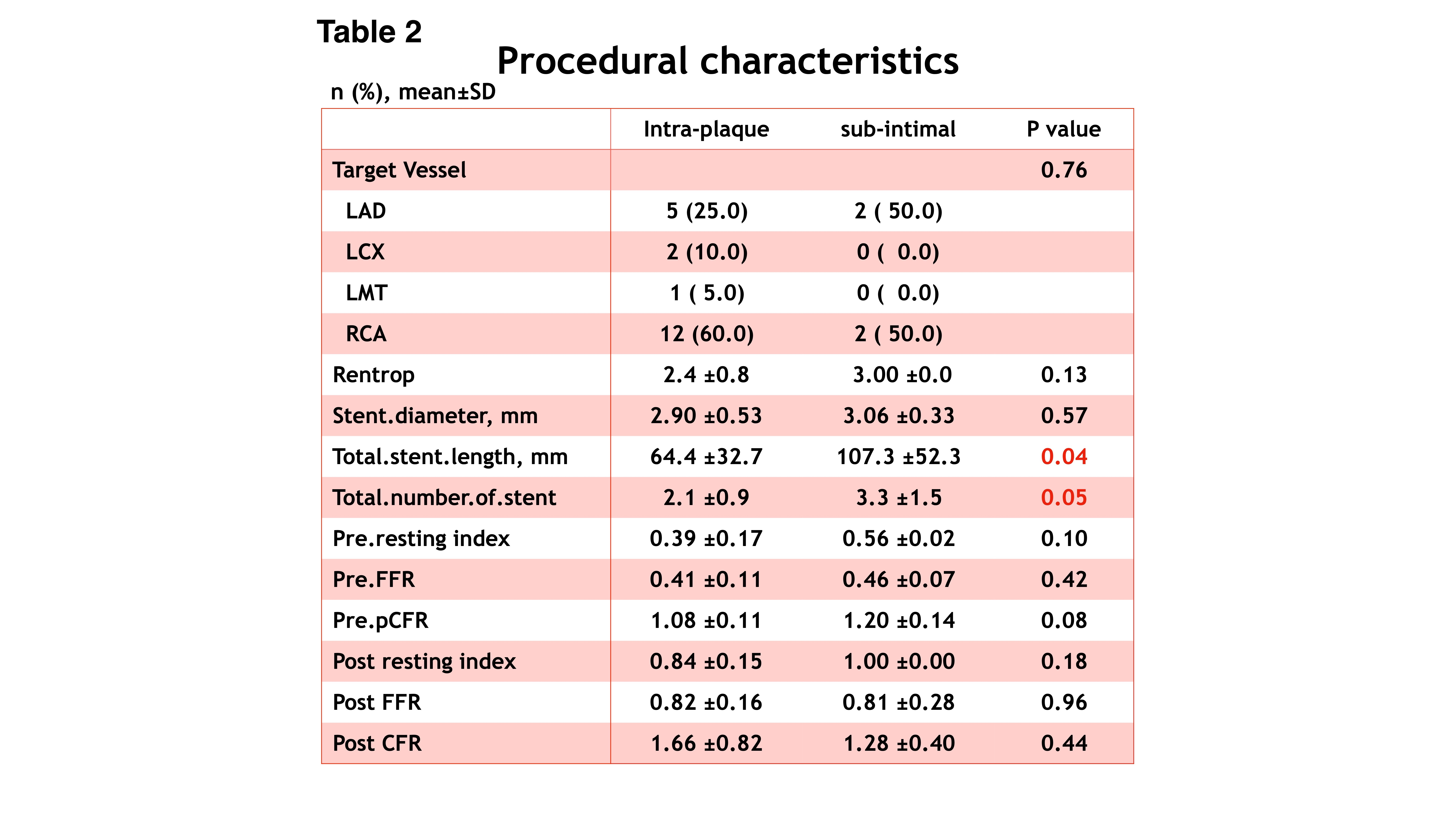
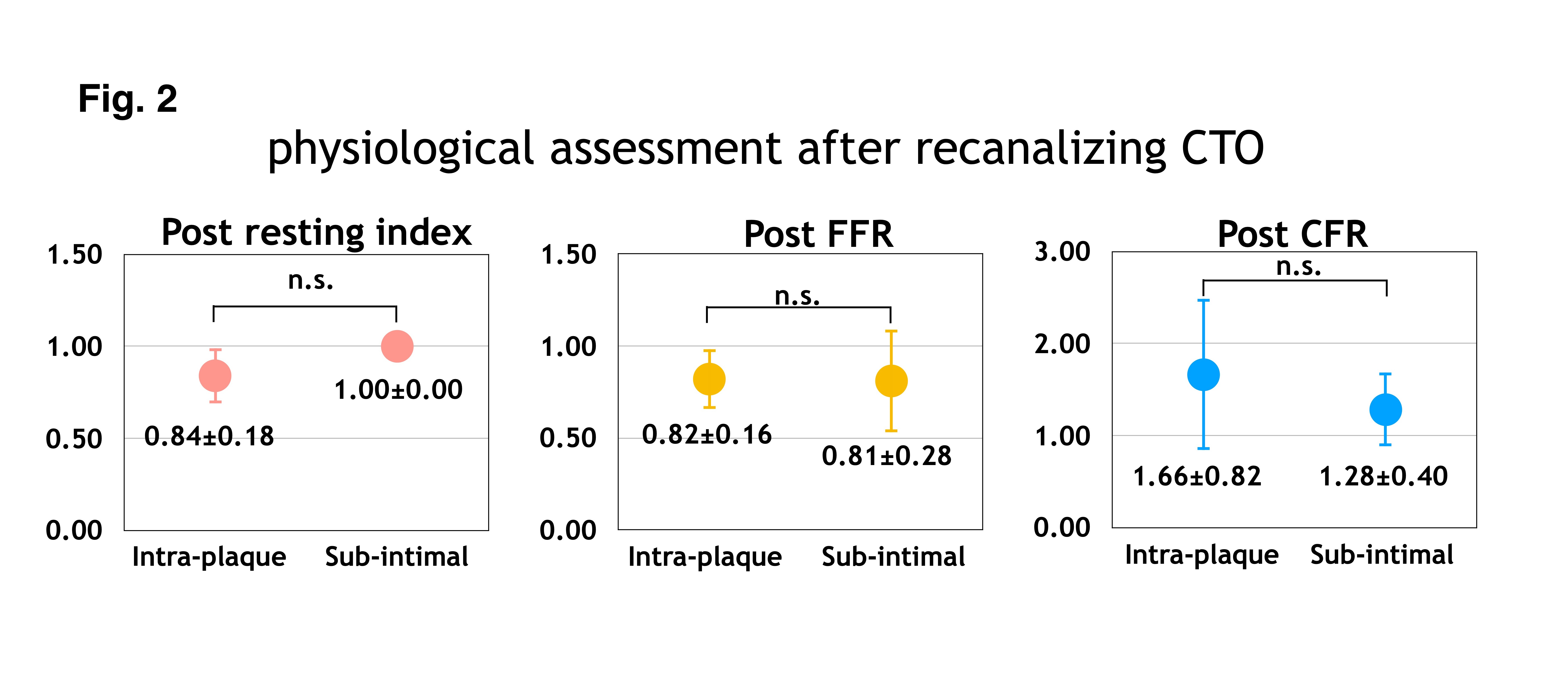
Post-procedural resting index (0.42 ± 0.17 vs. 0.86 ± 0.15, p<0.01), FFR(0.42 ± 0.11 vs. 0.82 ± 0.17, p<0.01) and pCFR(1.10 ± 0.12 vs. 1.61 ± 0.78, p<0.01) were significantly improved respectively (Fig.1). Although SI group had significantly high number of stents (2.1 ± 0.9 vs. 3.3 ± 1.5, p=0.05) and high number in total stent length (64.4 ± 32.7 mm vs. 107.3 ± 52.3 mm, p=0.04), post procedural resting index (0.84±0.15 vs. 1.00±0.00, p=0.18), FFR(0.82±0.16 vs. 0.81±0.28, p=0.95) and pCFR(1.66±0.82 vs. 1.28±0.40, p=0.44) weren’t statistically significant compared to T group (Talbe2, Fig.2).
   |
|
|
Conclusion:
Although sub-intimal tracking during CTO-PCI associated with high number of stents and stent length, sub-intimal stenting is a feasible strategy regarding to post-procedural physiological improvement compared to intra-luminal stenting,
|
|