Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
ABS20190928_0003
| Renal Insufficiency and Contrast Nephropathy | |
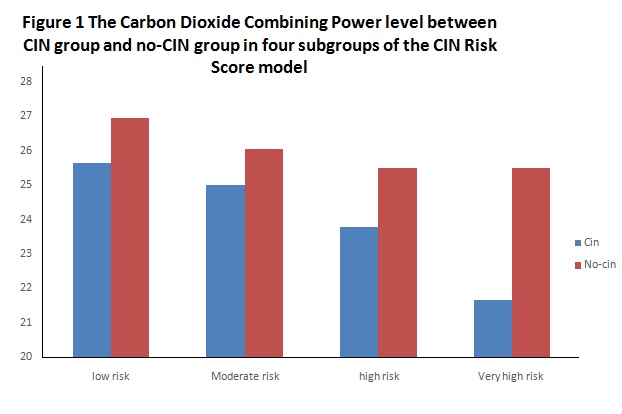
| Role of Carbon Dioxide Combining Power in Predicting Contrast-Induced Nephropathy in Patients Undergoing Emergency Percutaneous Coronary Intervention | |
| Geng Qian1, Qinhua Jin1 | |
| Chinese PLA General Hospital, China1 | |
|
Background:
Unknown remained in the relationship between Carbon Dioxide Combining Power (CO2-CP) and contrast-induced nephropathy(CIN), We aimed to investigate the role ofCO2-CP in predicting CIN in patients undergoing percutaneous coronary intervention (PCI).
|
|
|
Methods:
This retrospective observational research enrolled consecutive 1313 Non-ST segment elevation acute coronary syndrome (NSTE-ACS) patients undergoing emergency PCI. Admission CO2-CP levels were measured before PCI. We continuously monitored the serum creatinine (SCr) in perioperative period. CIN was defined as an increase in SCr at least 25% or 44.2 umol/L (0.5 mg/dL) within 3 days.
|
|
|
Results:
CIN occurred in 138 patients (10.53%). Compared with the no-CIN group, the CIN group have a significantly lower CO2-CP levels (25.19±3.79 vs 26.48±3.02 mmol/L, P<0.001).Multivariate logistic regression analysis showed that CO2-CP (OR=0.420, 95% CI0.257 to 0.686, P=0.001), heart failure (OR=2.167, 95% CI 1.475 to 3.185,P<0.001), anemia (OR=1.921, 95% CI 1.206 to 3.060, P=0.006), SCr(OR=1.914, 95% CI 1.016 to 3.606, P=0.045) and hypotension (OR=2.288,95% CI 1.416 to 3.697, P=0.001)were independent predictors of CIN. AndCIN group had a significant lower CO2-CP level in different risk groups [low-risk group (25.64±3.87 vs 26.96±2.79 mmol/L, P=0.001), moderate risk group (25.00±3.26 vs 26.05±2.98 mmol/L, P=0.021),high group(23.77±3.96 vs 25.49±3.22 mmol/L, P=0.023),very high group (21.65±5.36 vs 25.58±3.49 mmol/L, P=0.039)], and the CO2-CP level was significantly decreased with the increased risk of CIN.
 |
|
|
Conclusion:
This study showed low CO2-CP level was independently associated with an increased risk of CIN for patients with Non-ST egment elevation acute coronary syndrome.
|
|