
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-086
Prophylaxis ECMO-Supported Complex Percutaneous Coronary Intervention in Patient With Severe Left Ventricular Dysfunction and Severe Peripheral Vascular Disease
By Amy Jing Ling, Wei-Hsian Yin, Tien Ping Tsao, Yung-Tsai Lee
Presenter
Amy Jing Ling
Authors
Amy Jing Ling1, Wei-Hsian Yin1, Tien Ping Tsao1, Yung-Tsai Lee1
Affiliation
Cheng Hsin General Hospital, Taiwan1,
View Study Report
TCTAP C-086
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
Prophylaxis ECMO-Supported Complex Percutaneous Coronary Intervention in Patient With Severe Left Ventricular Dysfunction and Severe Peripheral Vascular Disease
Amy Jing Ling1, Wei-Hsian Yin1, Tien Ping Tsao1, Yung-Tsai Lee1
Cheng Hsin General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
D600555
Relevant Clinical History and Physical Exam
This 63 years old woman has history of ESRD under PD, diabetes mellitus type 2, hypertension and duodenal ulcer. She suffered from compressive chest pain which was accompanied with cold sweating and dyspnea on exertion. The symptoms could be relieved by sublingual NTG or rest. NSTEMI with CAD & TVD was diagnosed in previous hospital with LAD and RCA CTO PCI failure that CABG was suggested. Thus, she was transferred to our hospital for the second opinion.
Heart: RHB, systolic murmur over apex
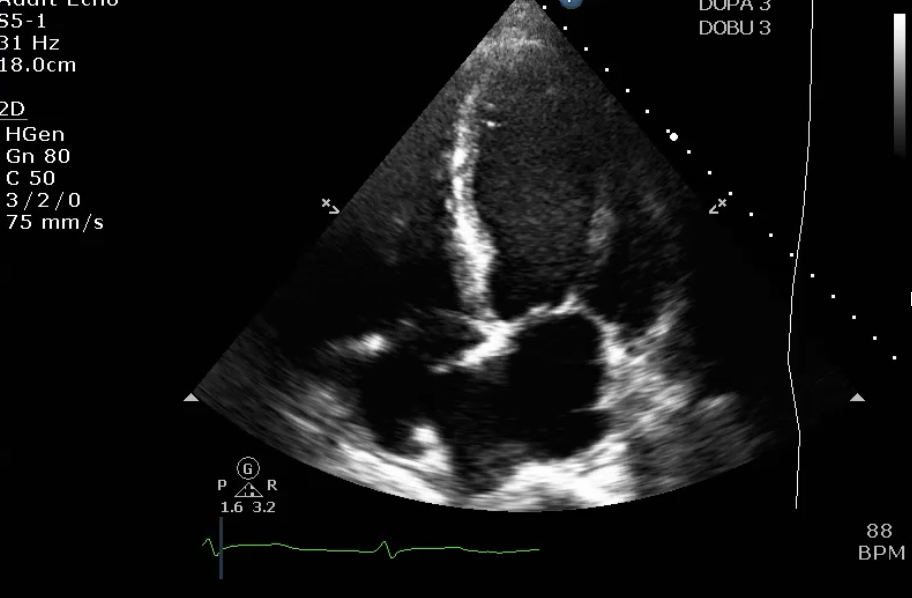
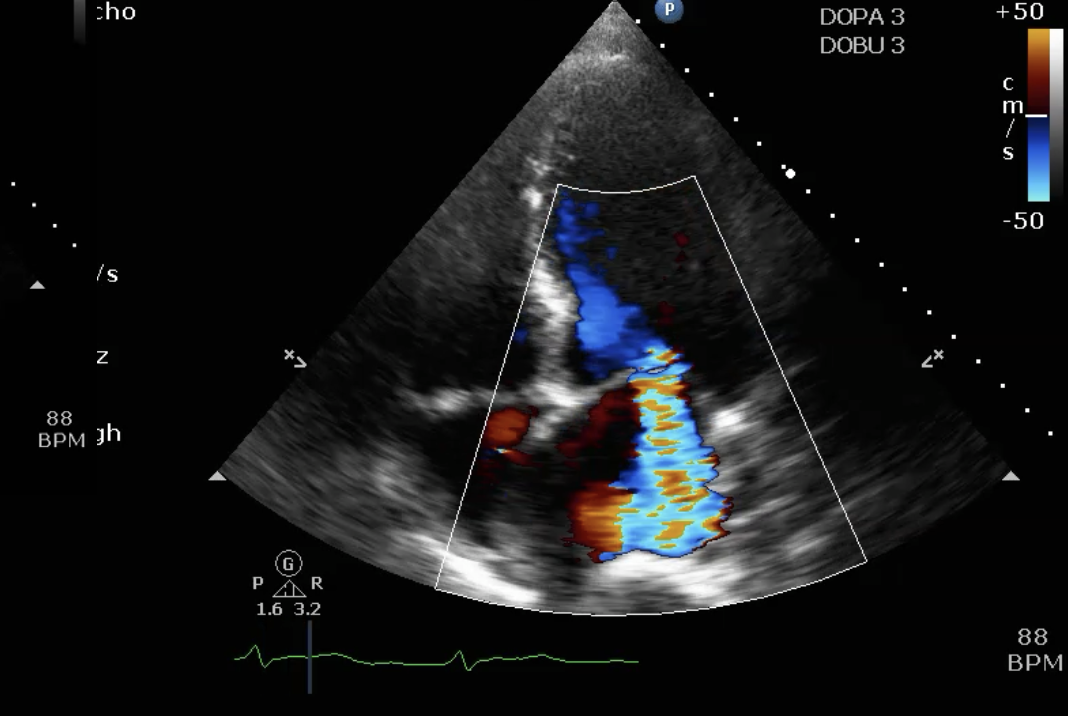
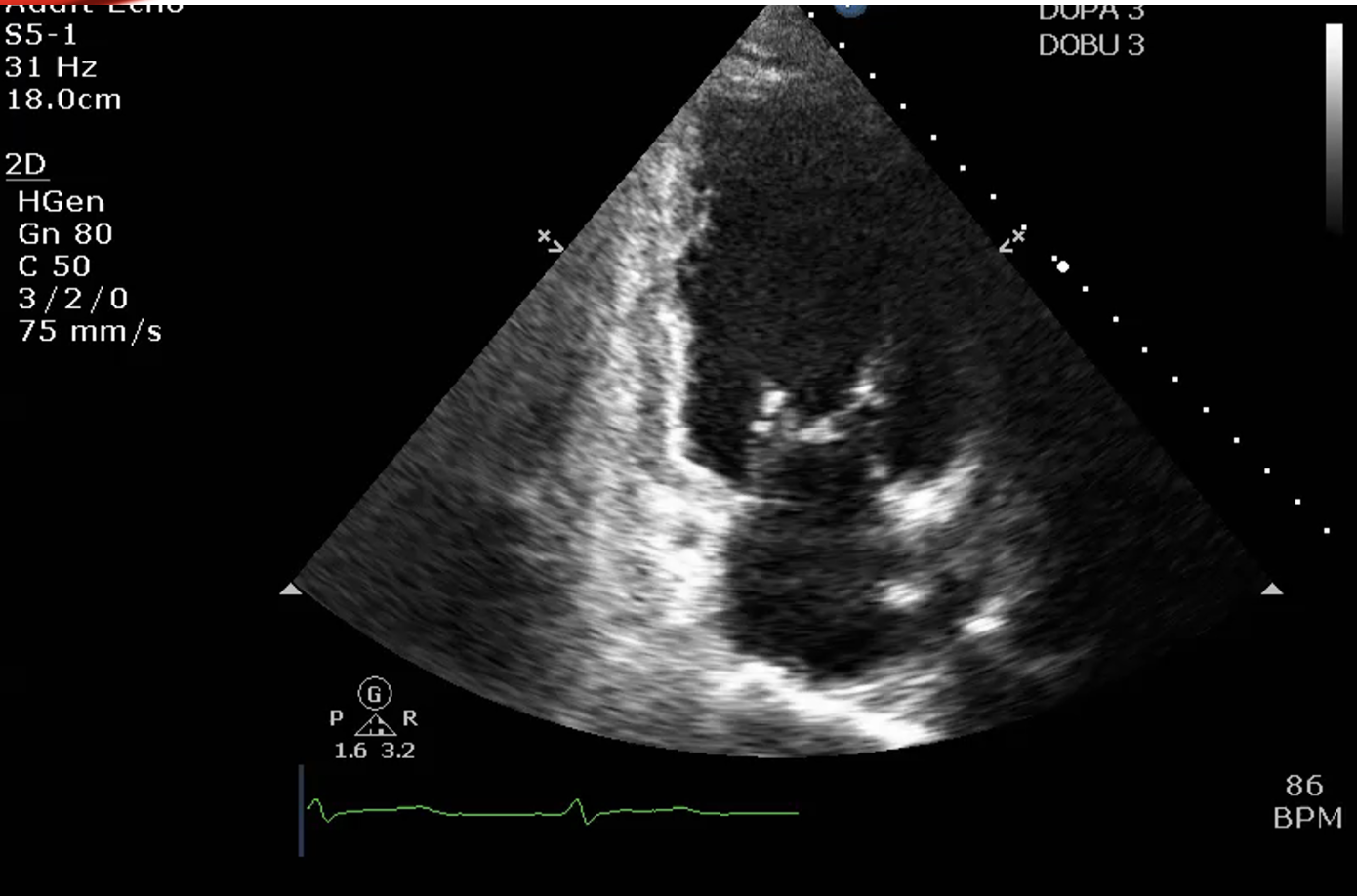
Relevant Test Results Prior to Catheterization
under dopamine 3mcg/kg/min and dobutamine 3mcg/kg/min,LVEF: 20%, severe MR, type IIIb, annulus diameter: 34 mmLV generalized hypokinesis middle to apical septal akinesistroponin-I: 3028.3 pg/mlCK-MB: 5.4 ng/ml
Relevant Catheterization Findings
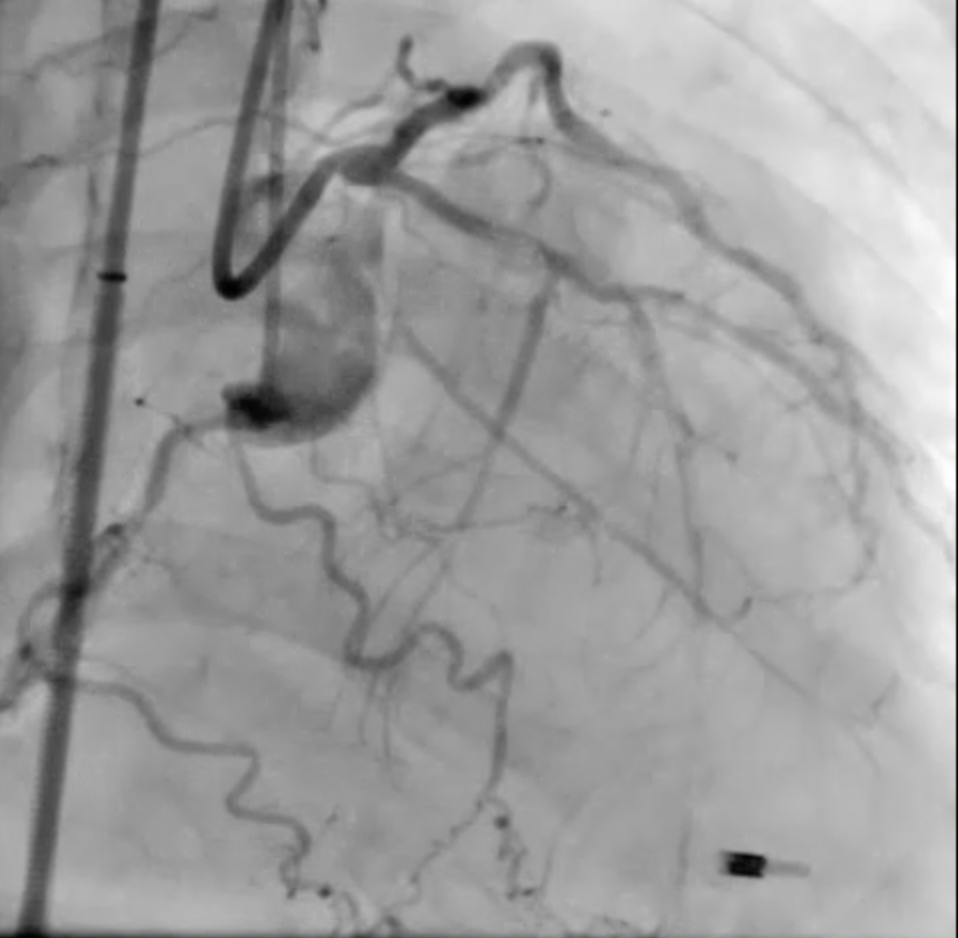
LAD-P 90-95% critical stenosis with heavy calcification, LAD-M 100% stenosis

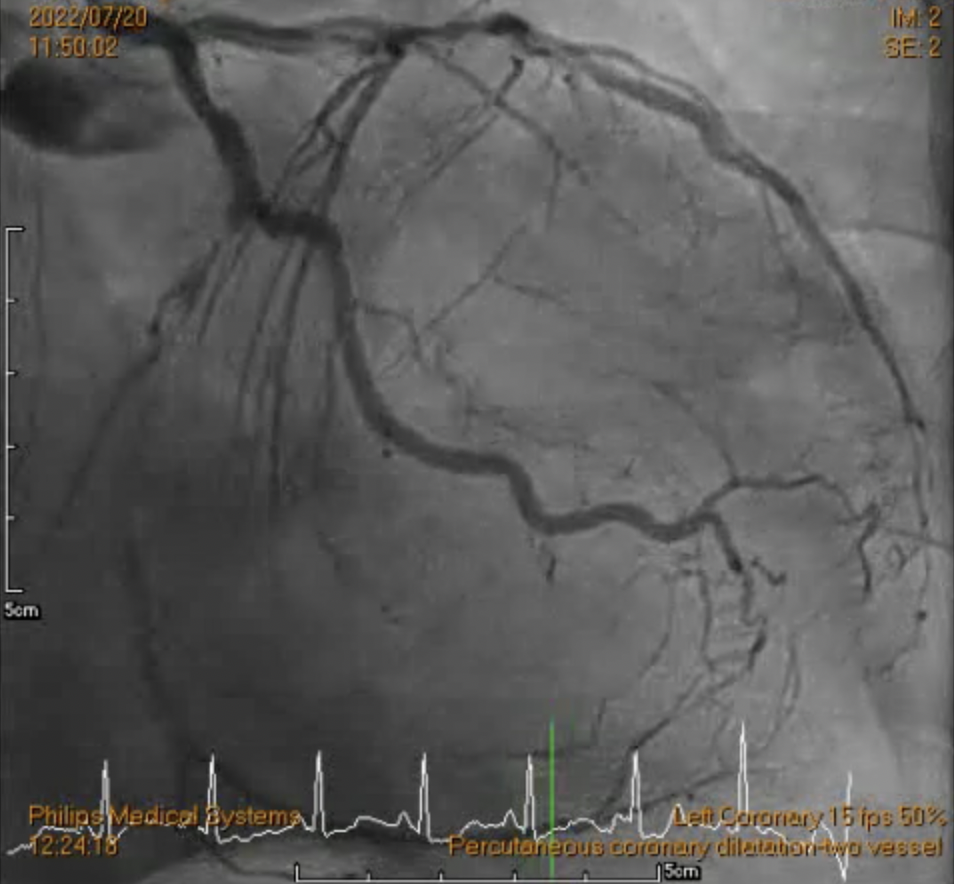
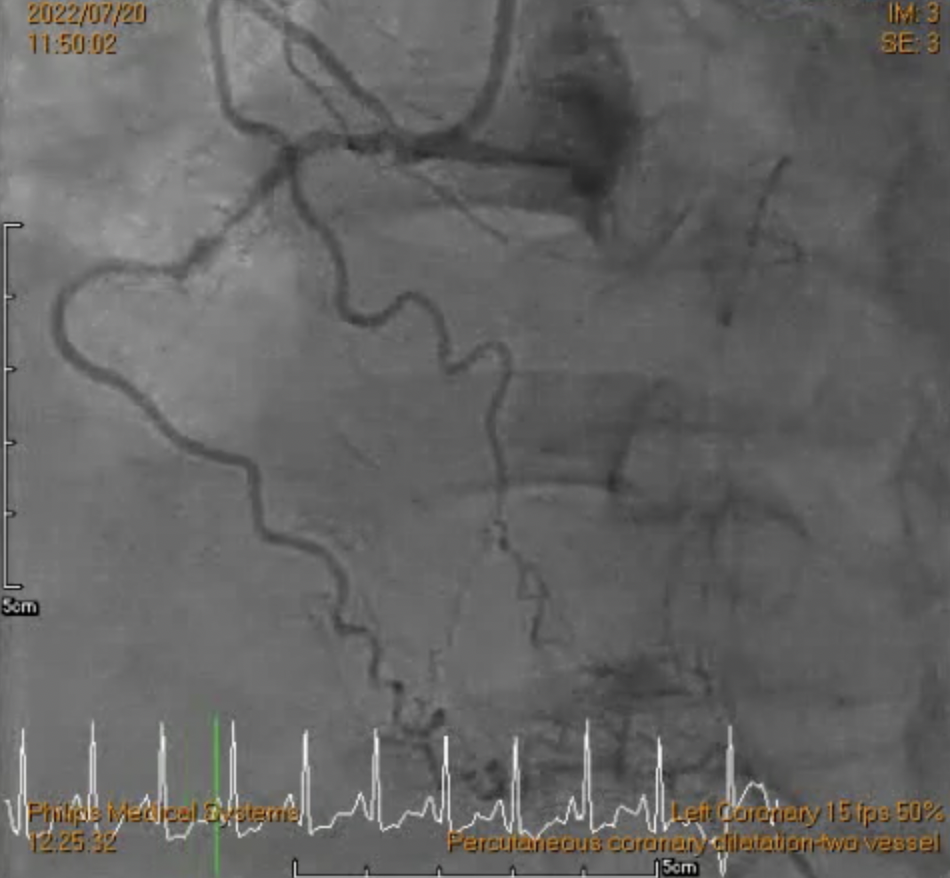
LCX-P CTO, collateral from OM
RCA-M heavy calcification with 100% stenosis, RV branch and conus branch collateral to LAD
Interventional Management
Procedural Step
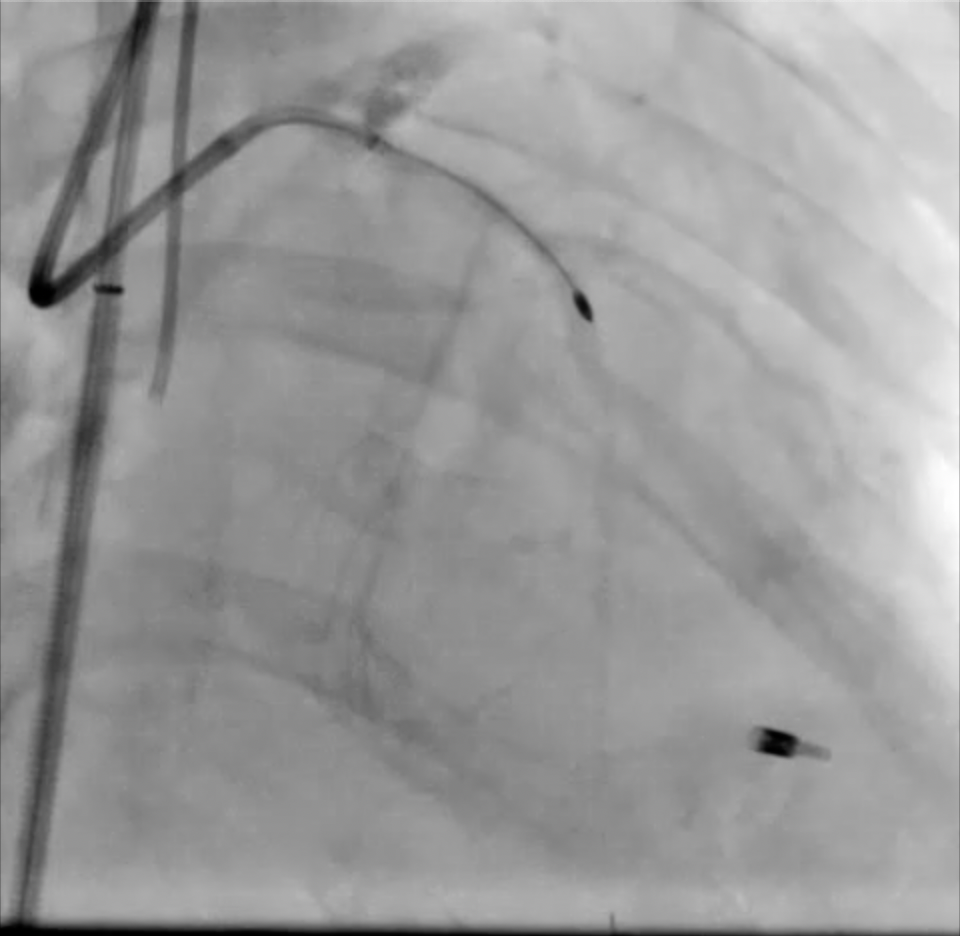
.After disscussion with the heart team, prophylaxis ECMO assisted LAD-M CTO PCI was suggested..Due to bilateral lower limbs severe peripheral artery disease, right subclavian artery was chosen for ECMO implantation..LMCA was engaged with EBU3.5/7F guiding catheter, and RCA was engaged with JR4/5F guiding catheter via Right subclavian artery(cut-down, puncture ECMO-A graft) for contralateral guiding.
.Wire escalation strategy with navigation of micro-catheter..Frequent grenadoplasty by using 1.0mm, 1.2 mm and 2.0 mm balloon..IVUS showed diffuse atherosclerotic plaque and calcification, with two separate 360 degree superficial calcium ring at LAD-P and LAD-M, and RVD is 2.5mm at LAD-M, 3.0mm at LAD-P..Rotational atherectomy were performed with pre-mount 1.5mm Rota burr in the Guidezilla II/7F extension catheter. Rotablation to LAD was done at 160,000 rpm..Shifted wire to Sionblue guide wire by using Finecross microcatheter and extension wire..POBA was performed with 2.5 x 15mm NC Emerge balloon at 12-16atm..Advanced Guideliner 6F extension catheter to LAD-M by using balloon anchor technique..2.5 x 38mm DES and 3.0 x 38mm DES were deployed from LAD-ostium to LAD-M..Post-dilatation with 2.5 x 15mm NC balloon at 12-20atm at LAD-M, and 3.0 x 15mm NC balloon at 16-20atm at LAD-P.
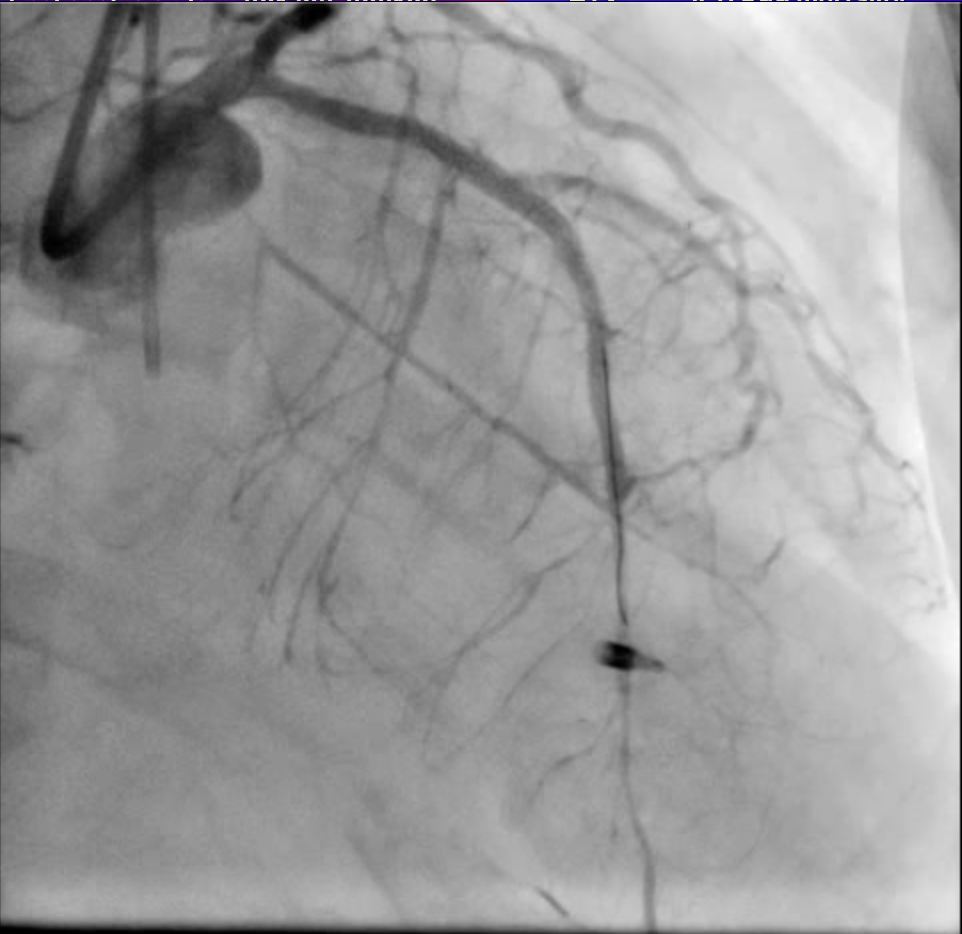
.Wire escalation strategy with navigation of micro-catheter..Frequent grenadoplasty by using 1.0mm, 1.2 mm and 2.0 mm balloon..IVUS showed diffuse atherosclerotic plaque and calcification, with two separate 360 degree superficial calcium ring at LAD-P and LAD-M, and RVD is 2.5mm at LAD-M, 3.0mm at LAD-P..Rotational atherectomy were performed with pre-mount 1.5mm Rota burr in the Guidezilla II/7F extension catheter. Rotablation to LAD was done at 160,000 rpm..Shifted wire to Sionblue guide wire by using Finecross microcatheter and extension wire..POBA was performed with 2.5 x 15mm NC Emerge balloon at 12-16atm..Advanced Guideliner 6F extension catheter to LAD-M by using balloon anchor technique..2.5 x 38mm DES and 3.0 x 38mm DES were deployed from LAD-ostium to LAD-M..Post-dilatation with 2.5 x 15mm NC balloon at 12-20atm at LAD-M, and 3.0 x 15mm NC balloon at 16-20atm at LAD-P.
Case Summary
Complex high risk percutaneous coronary intervention is challenging and frequently accompanied by hemodynamic instability through a mechanism of procedure-induced ischemia of the heart. Not only in cardiogenic shock patient or hemodynamic unstable patient, ECMO can be successfully used for hemodynamic support during elective high risk PCI. The patient will have better outcome than those patients who urgent need of ECMO during procedure without prophylaxis used. Echocardiogram follow up after 2 months later of coronary intervention showed the patient had preserved LV function with mild mitral regurgitation.