
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-104
Radial Artery as a Bailout for Coronary Stent Loss
By Erwin Mulia
Presenter
Erwin Mulia
Authors
Erwin Mulia1
Affiliation
Ahmad Yani Metro Hospital, Indonesia1,
View Study Report
TCTAP C-104
CORONARY - Complications (Coronary)
Radial Artery as a Bailout for Coronary Stent Loss
Erwin Mulia1
Ahmad Yani Metro Hospital, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Z
Relevant Clinical History and Physical Exam
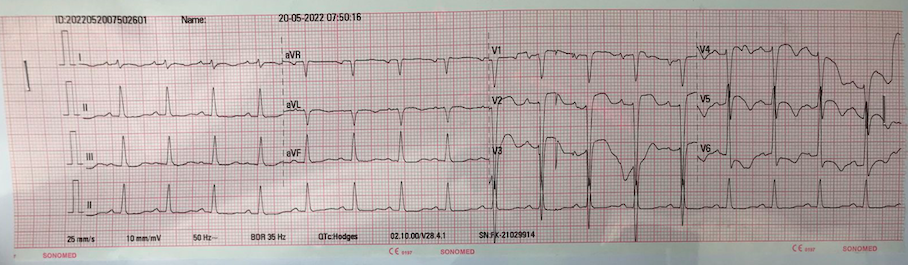
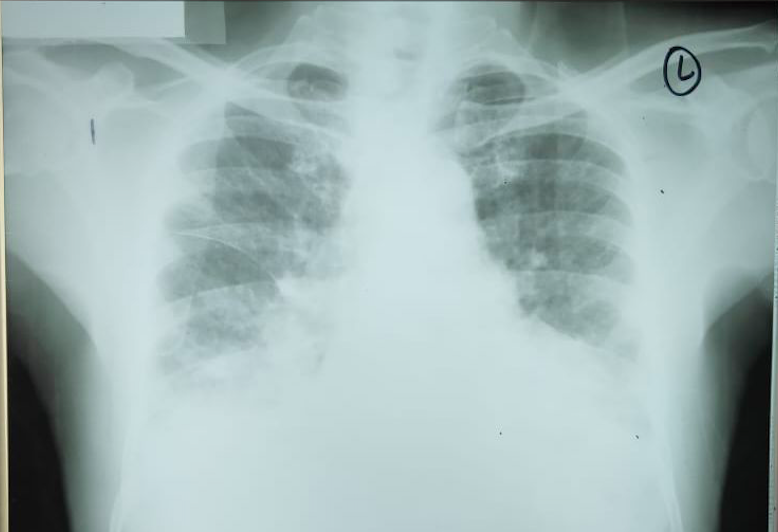
A 70 year old male came to our hospital with recurrent admission due to heart failure and unknown diabetes mellitus. Echocardiogram showed reduced left ventricular ejection fraction of 25 - 35% with regional wall motion abnormality involving LAD region. He was discharged with dual antiplatelet, candesartan 16 mg, bisoprolol 1.25 mg, simvastatin 20 mg, furosemide 40 mg, and insulin. He was planned for coronary angiogram and percutaneous coronary intervention as indicated.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
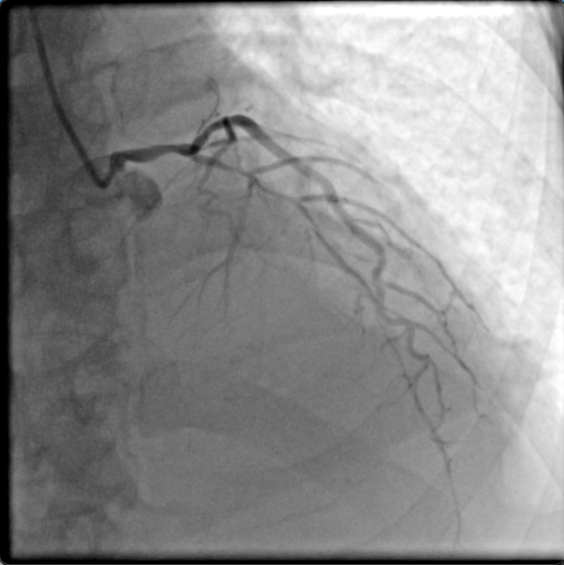
Using (TIG - 1) 5 Fr diagnostic catheter via 6 Fr radial sheathLeft Main Stem : severe stenosis at distal segment, minor irregularity at osteoproximal segmentLAD : diffusely diseased, severe stenosis from proximal to distal segmentLCx : minor irregularity at proksimal segmentRCA : severe stenosis at proximal segment, total occlusion at mid segment, distal is ipsilateral and contralateral collateralized


Interventional Management
Procedural Step
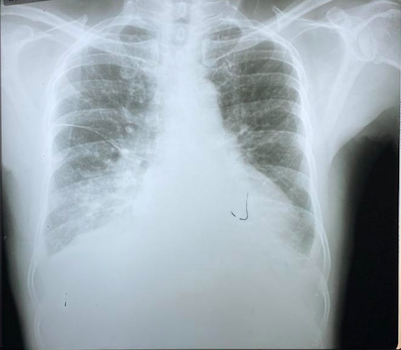
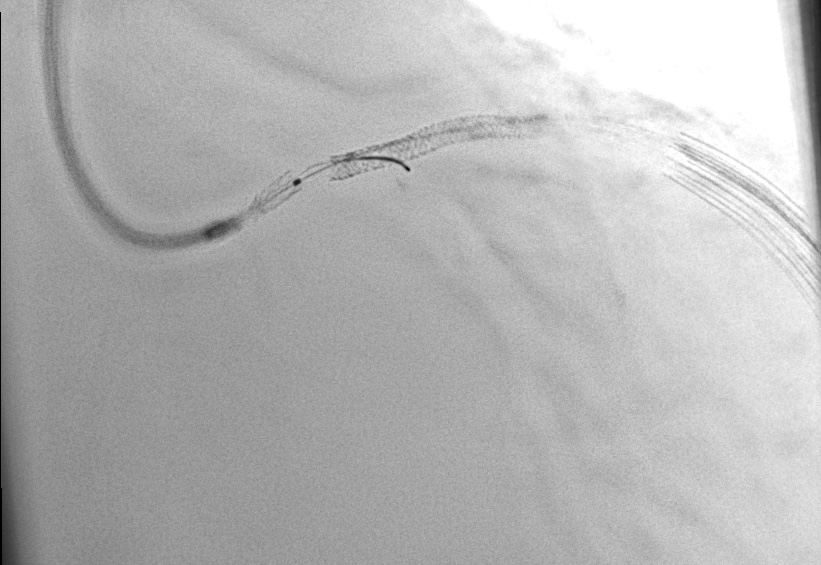
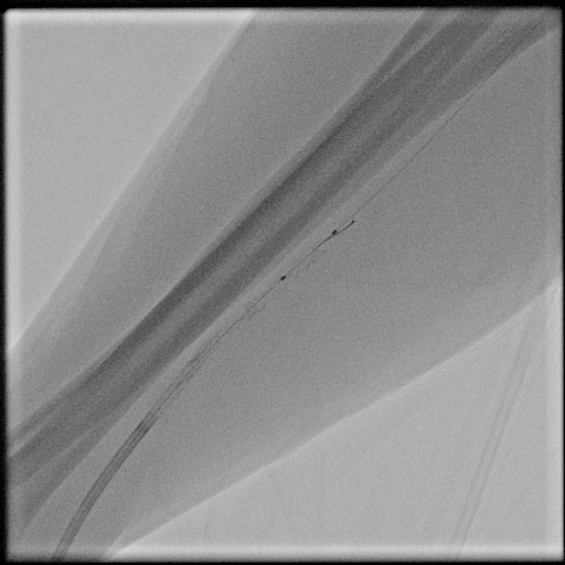
(XB 3.5) 6 Fr sidehole guiding catheter and (AnyReachP 1.0) guidewire was used to cannulate and wire the LAD. Predilation using semi compliant balloon (Sprinter Legend) 2.5 x 20 mm and mid left main to mid LAD lesion was stented using DES (Promus Premier Select) 2.75 x 32 mm. Second DES (Resolute Integrity) 2.5 x 18 mm was inserted to cover the mid LAD. Unfortunately, the passage of the second DES seemed to be stuck at the proximal end of the freshly implanted stent. Attempt to loose the stent resulted in lost stent from the stent balloon. We decided to perform multiple wires technique to retrieve the lost stent using additional 2 guidewires. Attempt to do so, resulted in broken guidewire in situ. So, another careful rewiring through the stent was performed, semi compliant balloon (Emerge) 2.5 x 15 mm was inserted and inflation technique was performed to anchor the stent and the whole system was pulled at once to bring the lost stent as near to the radial sheath as possible since the larger sheath was not available at the time. The lost stent was inflated sequentially and placed at radial artery. PCI was then continued through right femoral artery using 6 Fr femoral sheath, post dilation was performed using non compliant balloon (Emerge) 3.25 x 12 mm. New DES (Resolute Integrity) 2.25 x 18 mm was implanted distally (overlapped). Further dilation at distal LAD was performed using the last balloon stent. Radial duplex ultrasound showed mostly apposed patent stent.

Case Summary
Stent loss with coronary wire still in-situ is one of the possible complication. Many options to resolve can be done to overcome this complication such as small balloon inflation, crush, snaring, and multiple wiring techniques. Coronary wire position is one of the main issue to define before deciding the strategy to overcome this complication. In this patient, complication was due to stent loss in left main stem during stent stuck retrieval. It was finally dealt with multiple wiring technique and balloon inflation-pulling technique. Finally, the lost stent was able to be retrieved and was implanted at radial artery. Months after, staged PCI was performed safely in this patient.