
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-016
Primary PCI in Total Thrombotic Occlusion of the Left Main Coronary Artery Presenting as ST-Elevation Myocardial Infarction With Cardiogenic Shock
By Ibnu Adams
Presenter
Ibnu Adams
Authors
Ibnu Adams1
Affiliation
RSUD Banten, Indonesia1,
View Study Report
TCTAP C-016
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Primary PCI in Total Thrombotic Occlusion of the Left Main Coronary Artery Presenting as ST-Elevation Myocardial Infarction With Cardiogenic Shock
Ibnu Adams1
RSUD Banten, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Mrs B
Relevant Clinical History and Physical Exam
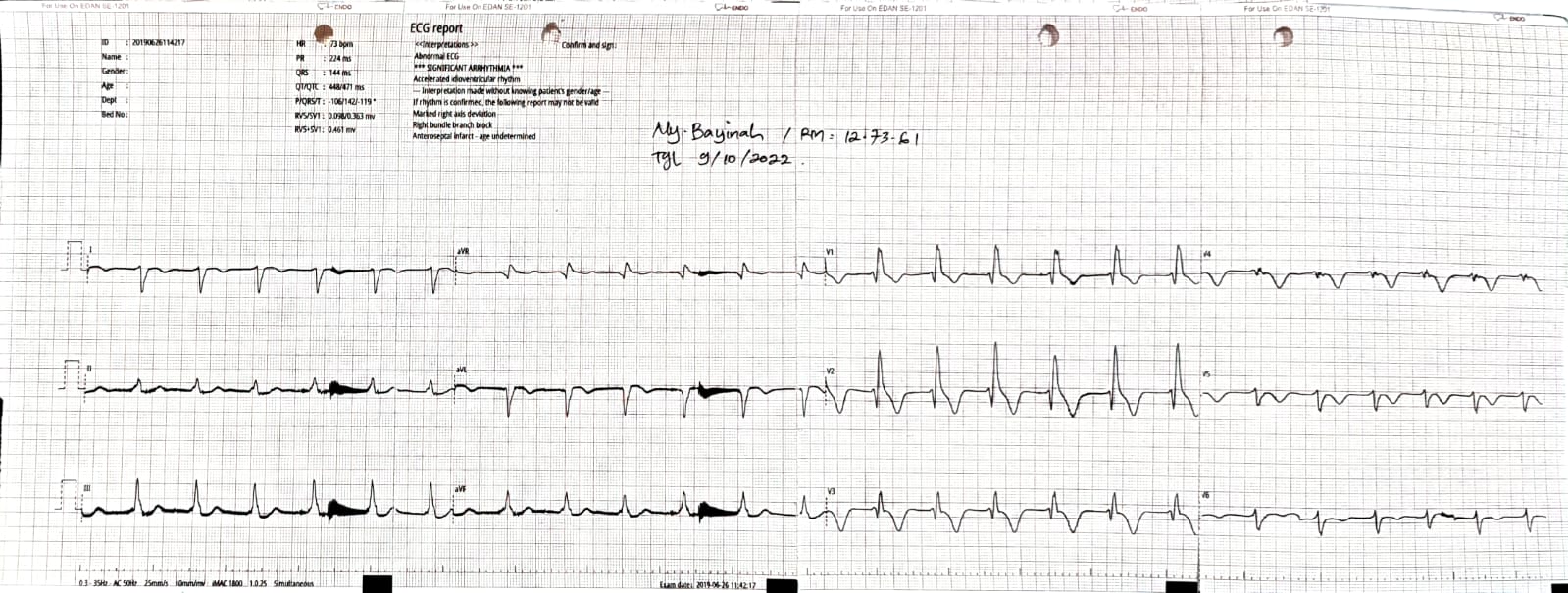
A 61 year-old woman presented with acute chest pain for 1 day and shortness of breath. Baseline ECG showed a new RBBB ST-elevation. Physical examination revealed crackles and hypotension. risk factor : hypertension
Relevant Test Results Prior to Catheterization
Troponin was elevated
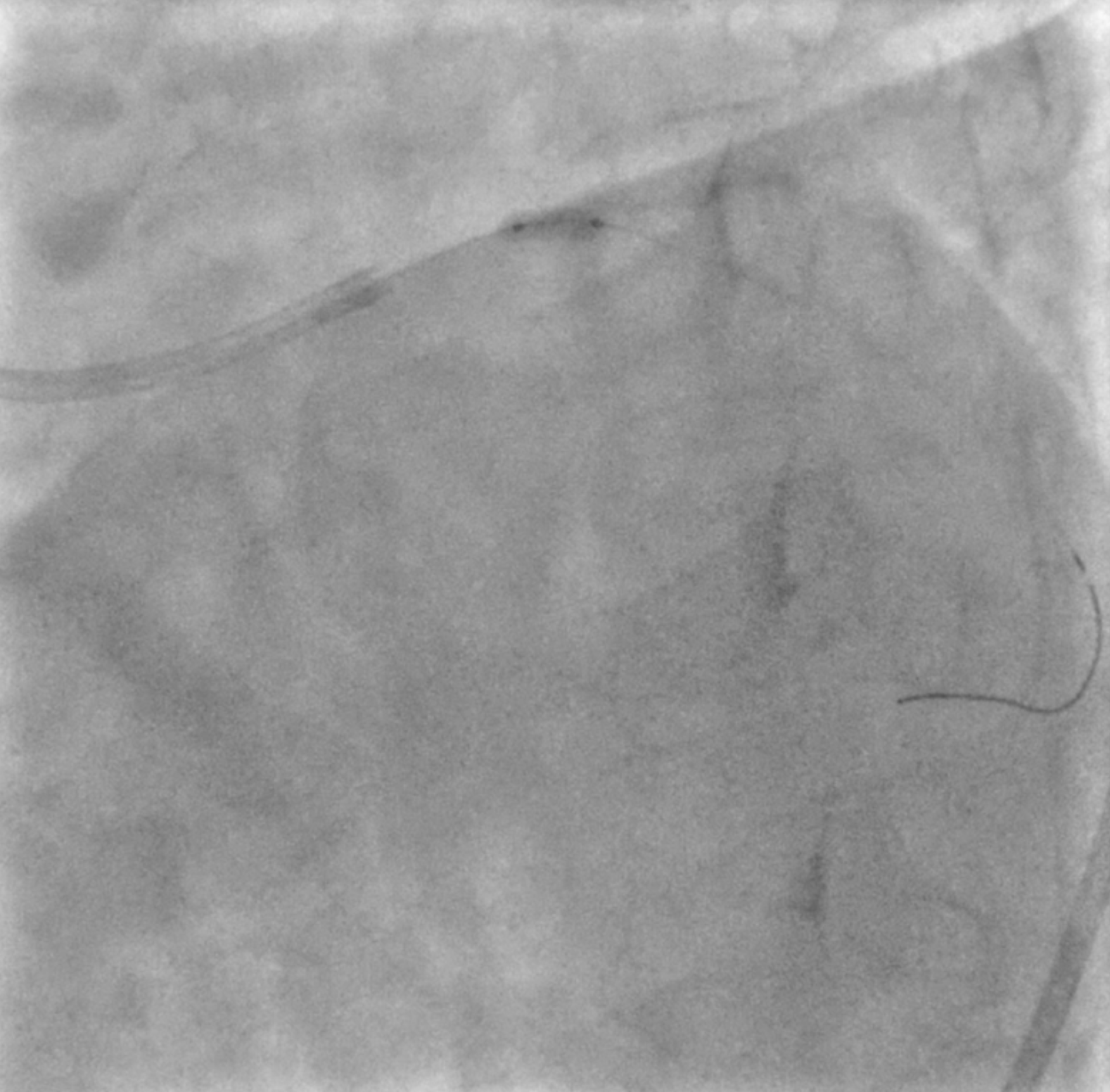
Relevant Catheterization Findings
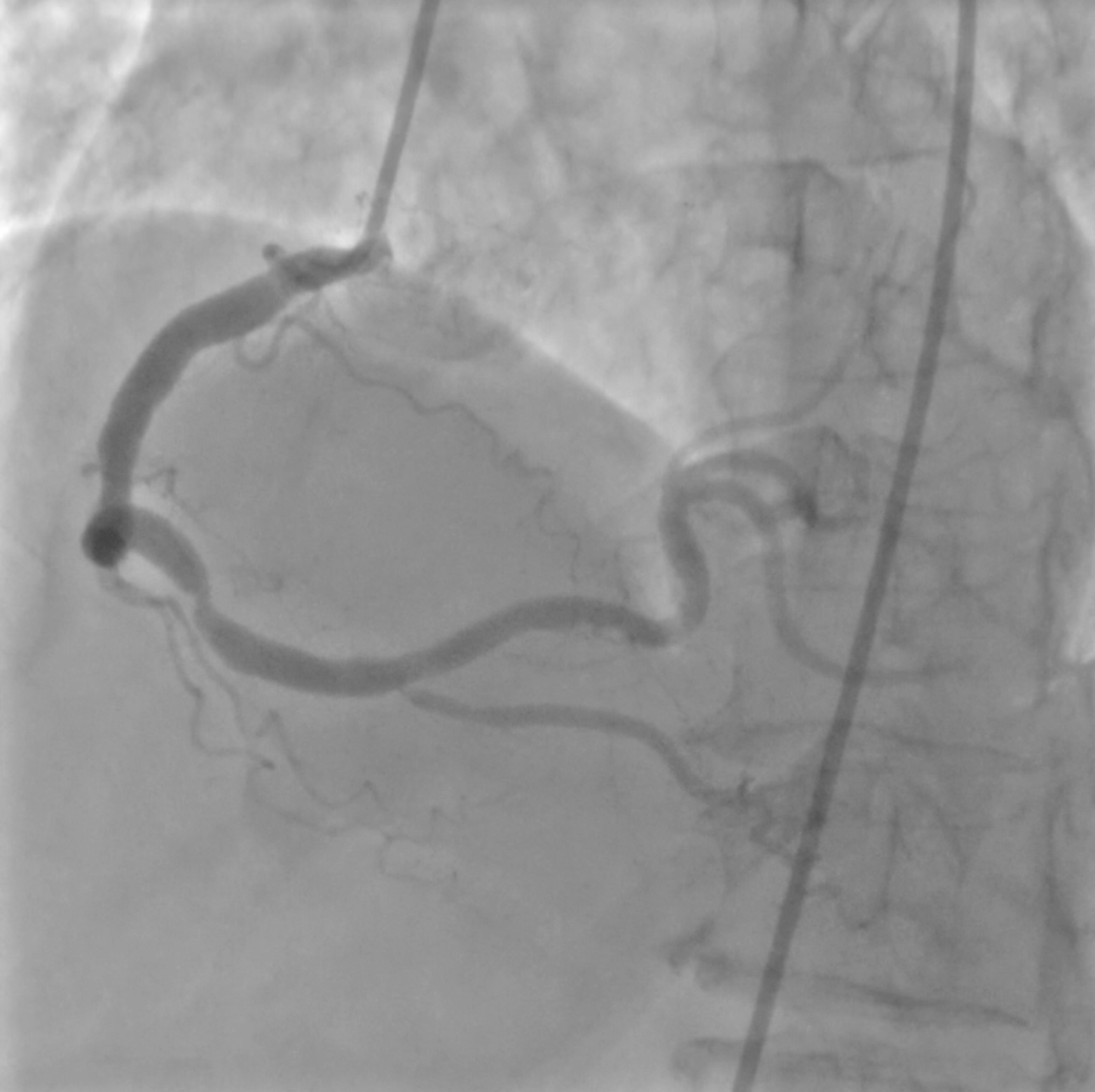
Angiography finding : Right dominant system. There was total thrombotic occlusion in distal LM and moderate stenosis in distal RCA. After aspiration thrombus and predilatation, contras injection showed diffuse and severe stenosis from proximal to mid LAD and CTO in ostial LCx.
Interventional Management
Procedural Step
A 7 Fr SBS 3,5 guiding catheter was engaged into LM ostium through right femoral artery. After workhorse guidewire was placed distally, thrombus aspiration was performed twice using an Aspiration Catheter APT followed by predilatation with a 2,5x15 mm semi compliance balloon in proximal LAD and inflated up to 18 atm. Contras injection showed TIMI 3 flow, LCx was not visible and guidewire was located in distal Diagonal, so another guidewire was placed in distal LAD and guidewire in distal Diagonal was pulled out. IVUS evaluation showed mixed plaque with lipid dominance in proximal LAD, distal reference diameter 2,75 mm in mid LAD, proksimal reference diameter 3,5 mm in proximal LAD and LM diameter was 4,0 mm. A 3,0/38 mm DES was placed in proximal-mid LAD and inflated under nominal pressure. The 2nd stent, a 3,5/28 mm DES was placed in ostial LM-proximal LAD in an overlapping manner and inflated to nominal pressure. Post dilatation was done with a 4,0x15 mm non compliance balloon inflated at 18 atm in LM. IVUS evaluation post stenting showed no stent edge dissection, well apposed and expanded stents, MSA in proximal LAD was 8,6 mm2 and MSA in LM was 12,3 mm2. Final angiogram showed TIMI 3 flow.

Case Summary
Total thrombotic occlusion in distal Left main with clinical presentation of STEMI new RBBB and cardiogenic shock was successfully managed by IVUS guided-Primary PCI with 2 DES stents in ostial LM to mid LAD