
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-088
Menacing CTO and Calcium in Severe LV Dysfunction- A Chip Case at Every Step
By Richa Sharma
Presenter
Richa Sharma
Authors
Richa Sharma1
Affiliation
Shri Mahant Indiresh Hospital, Dehradun, India1,
View Study Report
TCTAP C-088
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
Menacing CTO and Calcium in Severe LV Dysfunction- A Chip Case at Every Step
Richa Sharma1
Shri Mahant Indiresh Hospital, Dehradun, India1,
Clinical Information
Patient initials or Identifier Number
SS
Relevant Clinical History and Physical Exam
660year old hypertensive malep/w c/o AOE II, DOE II since 2-3yrs, increased since one month to NYHA III.
Relevant Test Results Prior to Catheterization
Stress Thallium : s/o viable RCA and LAD territories.
Relevant Catheterization Findings
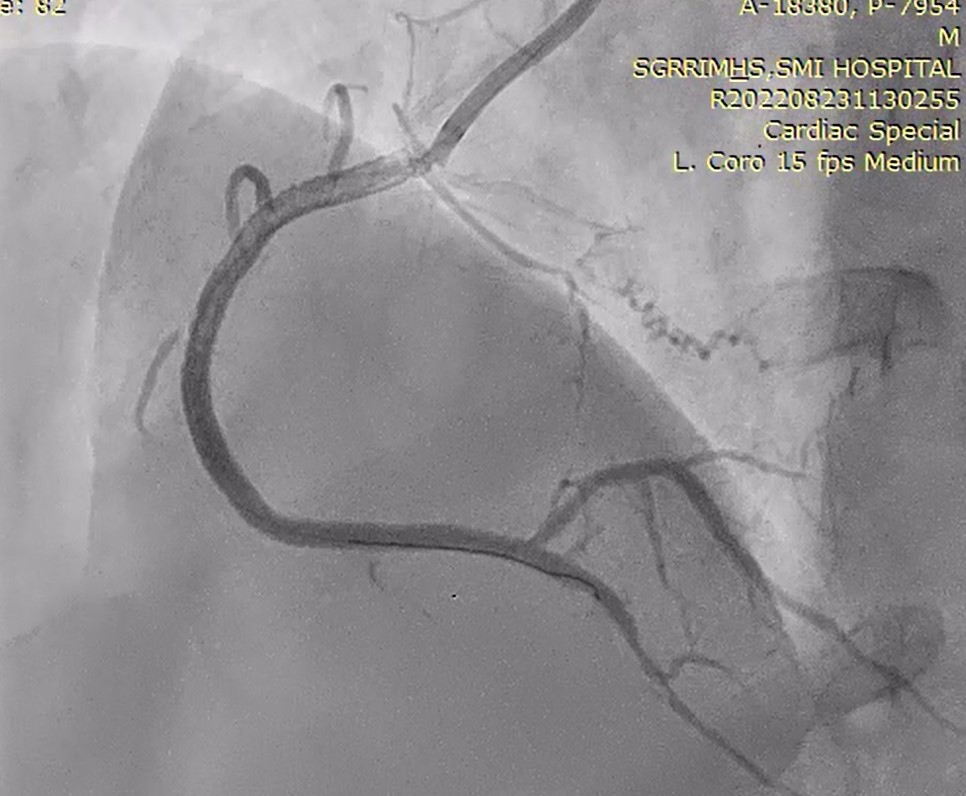
CAG was done via right radial route, s/o:Mild plaquing in LMCA shaft; Proximal to Mid LAD long lesion with 90% stenosis, heavily calcific vessel; LCx 100% CTOMid RCA 100% CTO (retrograde collaterals from LAD to RCA) Since stress thallium s/o viable LAD & RCA territories, decision to revascularize the same.
PLAN A- antegrade approach with a CTO wire upfront with microcatheter supportPLAN B- retrograde approach after first revascularizing LAD

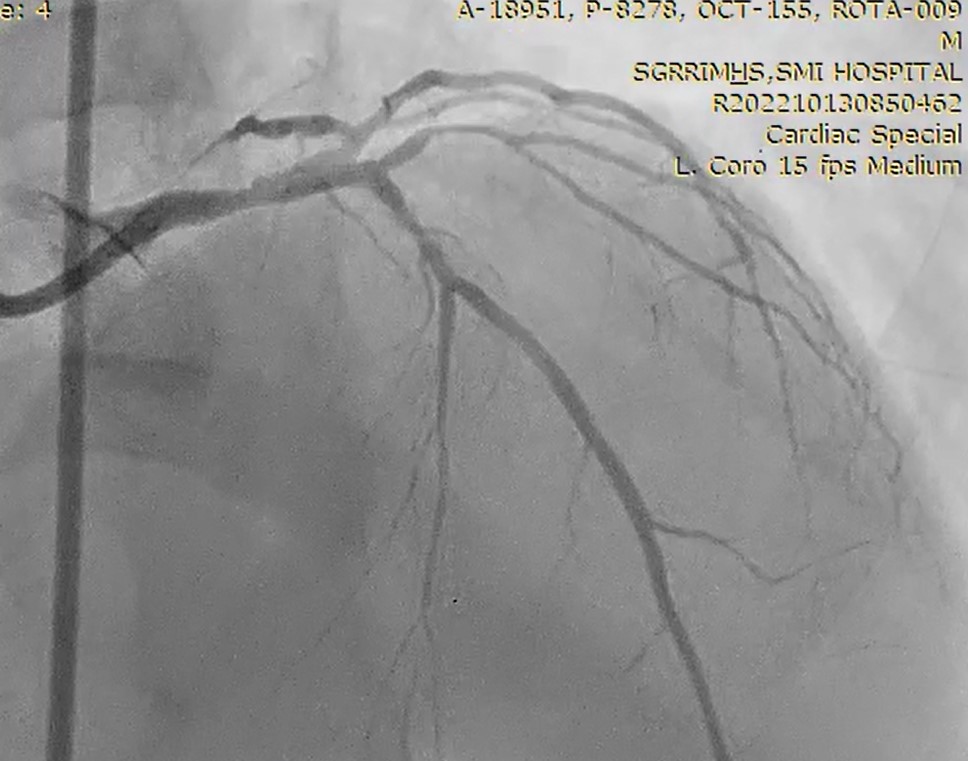
PLAN A- antegrade approach with a CTO wire upfront with microcatheter supportPLAN B- retrograde approach after first revascularizing LAD
Interventional Management
Procedural Step
PTCA toRCA
B/l Femoral artery access
7F AL-1/3.5 to hook RCA
EBU 3.5/6F hooked to left system


B/l Femoral artery access
7F AL-1/3.5 to hook RCA
EBU 3.5/6F hooked to left system
Case Summary
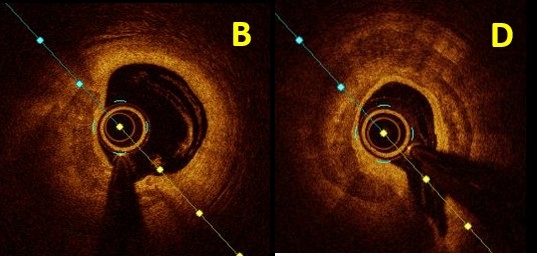
Assessing calcium and doing a proper bed preparation with various available modalities is extremely important for proper apposition and expansion of stent and preventing stent failure rates. Various tools to menace the tough calcium like cutting balloons, IVL, rotablation, OPN NC should be present in the cath lab while performing such a case. OCT is a better tool to assess calcium.