
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-049
Streamlined Reversed Wire Technique Using a Single-Lumen Angulated Microcatheter
By Yuen Fung Yiu, Raymond Chi Yan Fung
Presenter
Yuen Fung Yiu
Authors
Yuen Fung Yiu1, Raymond Chi Yan Fung1
Affiliation
Princess Margaret Hospital, Hong Kong, China1,
View Study Report
TCTAP C-049
CORONARY - Bifurcation/Left Main Diseases and Intervention
Streamlined Reversed Wire Technique Using a Single-Lumen Angulated Microcatheter
Yuen Fung Yiu1, Raymond Chi Yan Fung1
Princess Margaret Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
YTC
Relevant Clinical History and Physical Exam
YTC is a 78-year-old lady, with a history of type two diabetes and hypertension. She was admitted to our hospital for inferior ST elevation myocardial infarction, for which she was given intravenous thrombolytic therapy. Percutaneous coronary intervention (PCI) was done in the next morning and the culprit lesion over left circumflex artery were treated with two drug-eluting stents. She was scheduled for staged PCI for the left coronary artery lesions two weeks later.
Relevant Test Results Prior to Catheterization
Echocardiogram showed normal LV systolic function and valvular function.
Relevant Catheterization Findings
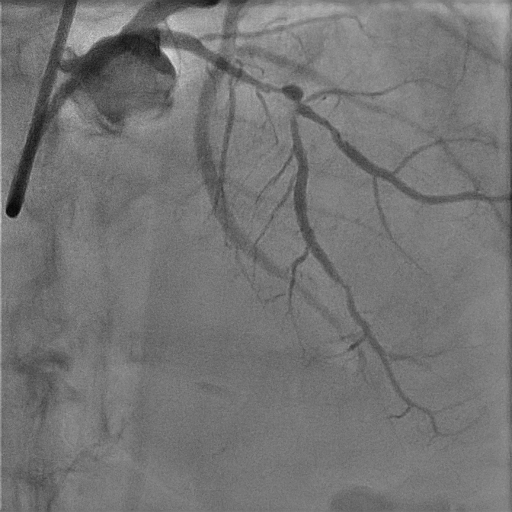
Coronary angiogram showed diffuse severe stenosis over middle segment of the LAD, with 90% stenosis just before and after a sizeable diagonal branch. Left main was unremarkable and the recently implanted stents in LCX were patent. The RCA was non-dominant and small in diameter.
Interventional Management
Procedural Step
The ostium of LM was engaged with a 7 Fr EBU 3.5 catheter. A workhorse wire could not be delivered to distal part of the LAD as it selected towards the diagonal branch. We tried to wire the LAD with the assistance of an angulated microcatheter pulled back from the diagonal branch, without success. It was decided to attempt reverse wiring of the LAD from diagonal branch in view of the extreme angulation of the LAD takeoff. The usual reverse wiring technique (RWT) facilitated by dual lumen catheter was not used, as the bulky hairpin wire and catheter complex was unlikely to negotiate through the tight proximal lesion successfully without predilation.


Case Summary
This case illustrated that a single lumen angulated microcatheter would be useful for wiring a side or main branch with a very acute angle. It could assist wiring directly or indirectly by reverse wiring technique. Compared to the more commonly used dual lumen catheter-assisted RWT, the single lumen angulated microcatheter has the advantage of a better crossing profile. In cases with severe stenosis proximal to the bifurcation, this technique can circumvent the need of pre-dilation that may risk compromising the opposite branch.