
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-031
Intra Coronary Thrombolysis Assisted Primary PCI to RCA in a Patient of Inferior Wall MI With Complete Heart Block, LV Failure and Renal Dysfunction
By Dileep Kumar Tiwari, Amjad Ali
Presenter
Dileep Kumar Tiwari
Authors
Dileep Kumar Tiwari1, Amjad Ali2
Affiliation
Baderiya Metroprime Hospital, India1, Sagar Multispeciality Hospital, India2,
View Study Report
TCTAP C-031
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Intra Coronary Thrombolysis Assisted Primary PCI to RCA in a Patient of Inferior Wall MI With Complete Heart Block, LV Failure and Renal Dysfunction
Dileep Kumar Tiwari1, Amjad Ali2
Baderiya Metroprime Hospital, India1, Sagar Multispeciality Hospital, India2,
Clinical Information
Patient initials or Identifier Number
JB
Relevant Clinical History and Physical Exam
A 71-year-old gentleman was brought to the emergency room with complaints of retrosternal chest pain and uneasiness for the last 14 hours and one episode of fainting followed by severe shortness of breath for two hours. On examination, he was dyspneic, his pulse rate was 36 bpm, BP was 160/100 mmHg, and SPO2 was 87% at room air. The JVP was raised and had bilateral crepitations on chest examination. The other systemic examination was unremarkable.
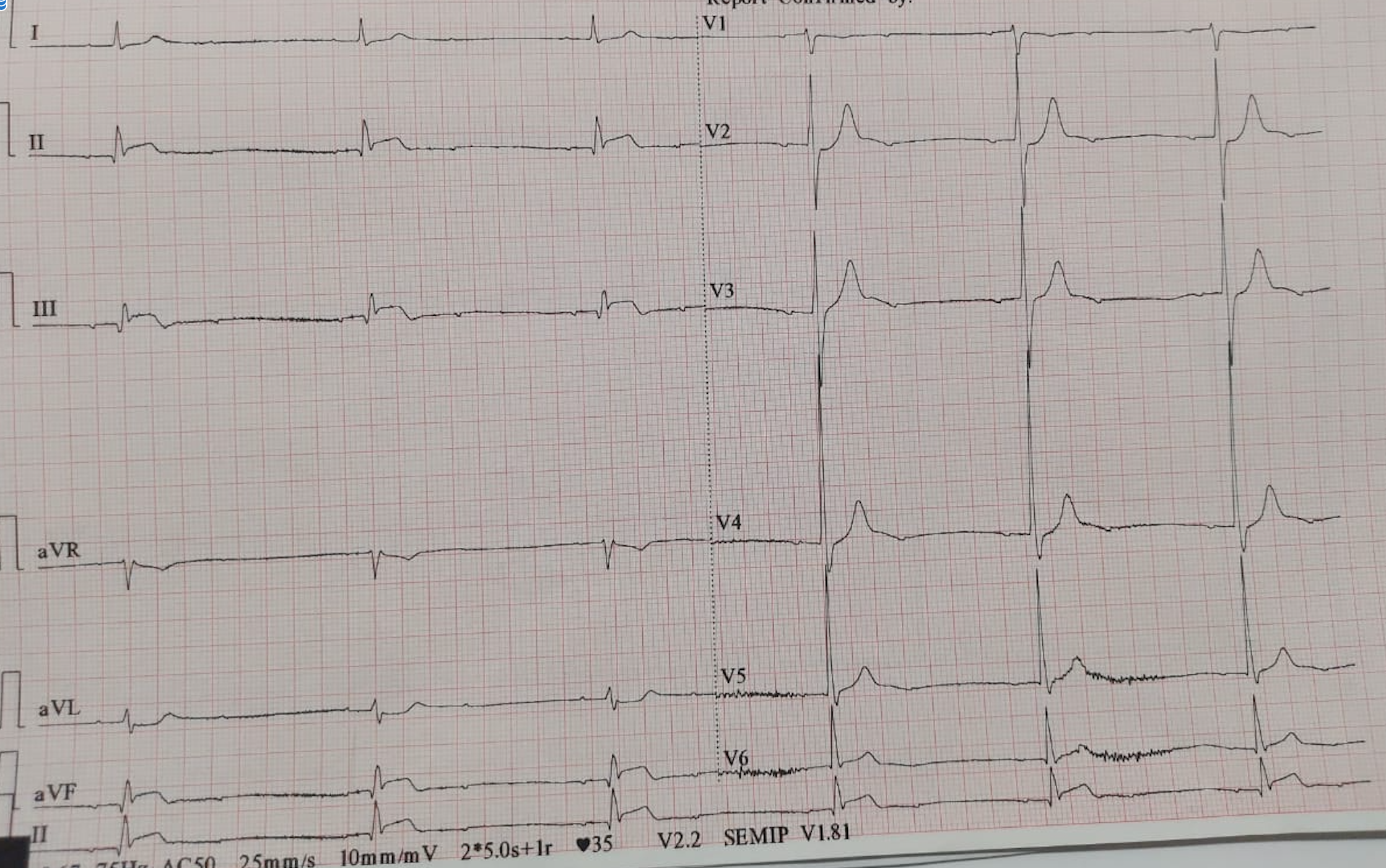
Relevant Test Results Prior to Catheterization
The ECG showed CHB with ST Elevation Inferior Wall MI. The echocardiogram suggested multi segments RWMA with LVEF 35%. His haemoglobin was 12.0 gm/dL, Creatinine 2.83 mg/dL, Potassium 6.3 mmol/L and NT pro-BNP was 8374 pg/mL. He was intubated and put on a ventilator. Other than the symptomatic treatment, loading doses of Ticagrelor 180 mg, Disprin 325 mg and Atorvastatin 80 mg were given. After taking written high-risk-informed consent, the patient was shifted to the catheterization laboratory.
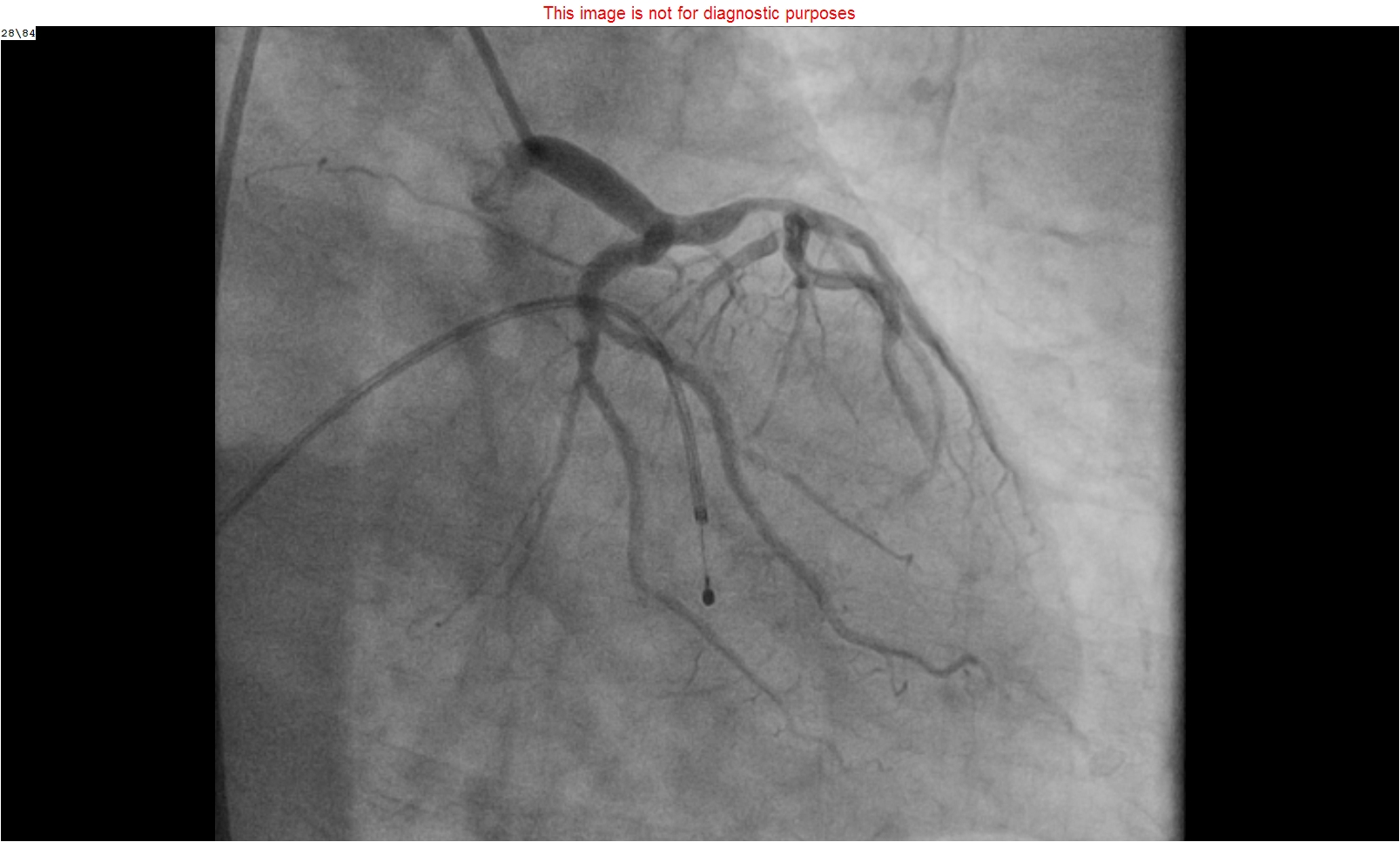
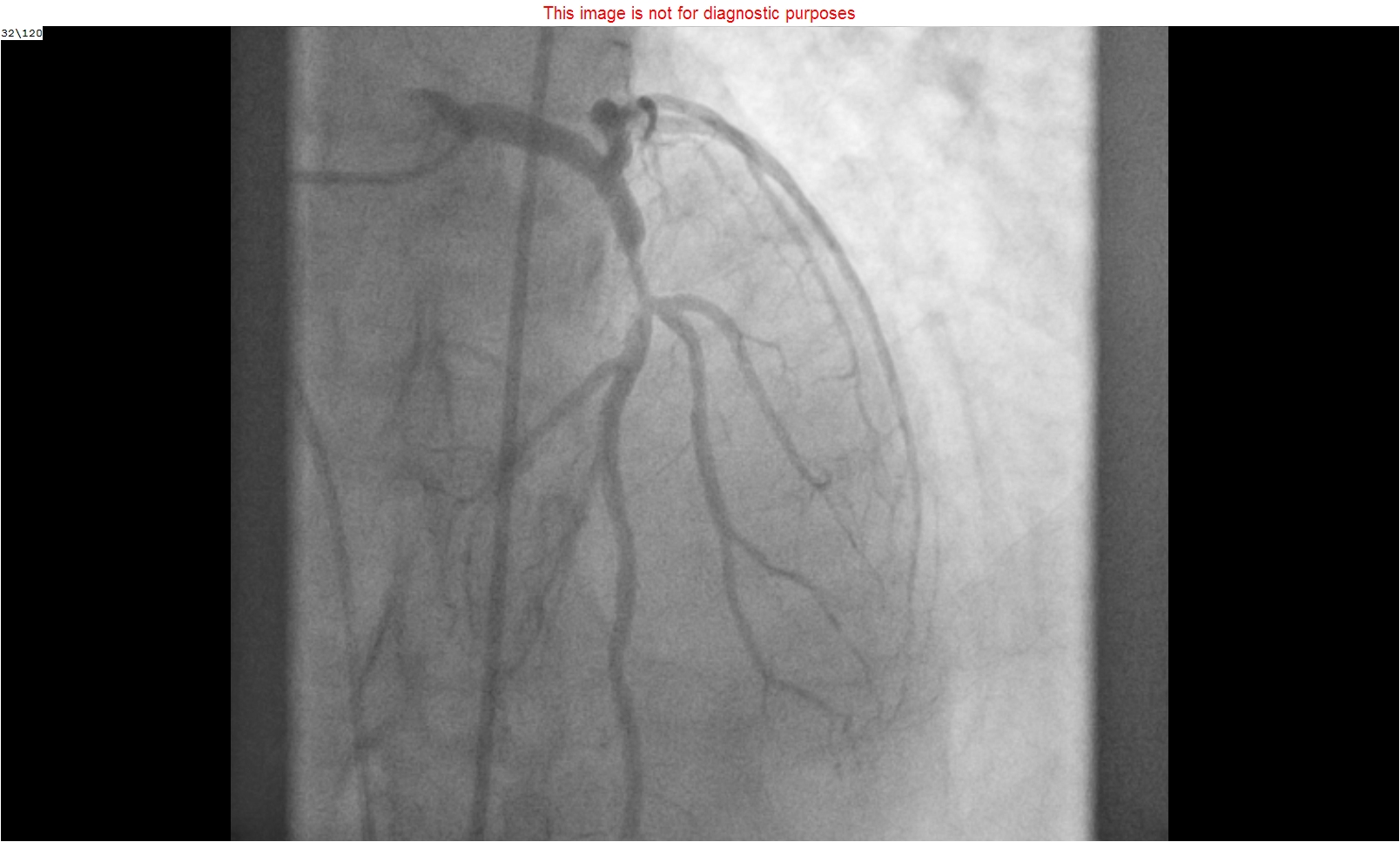
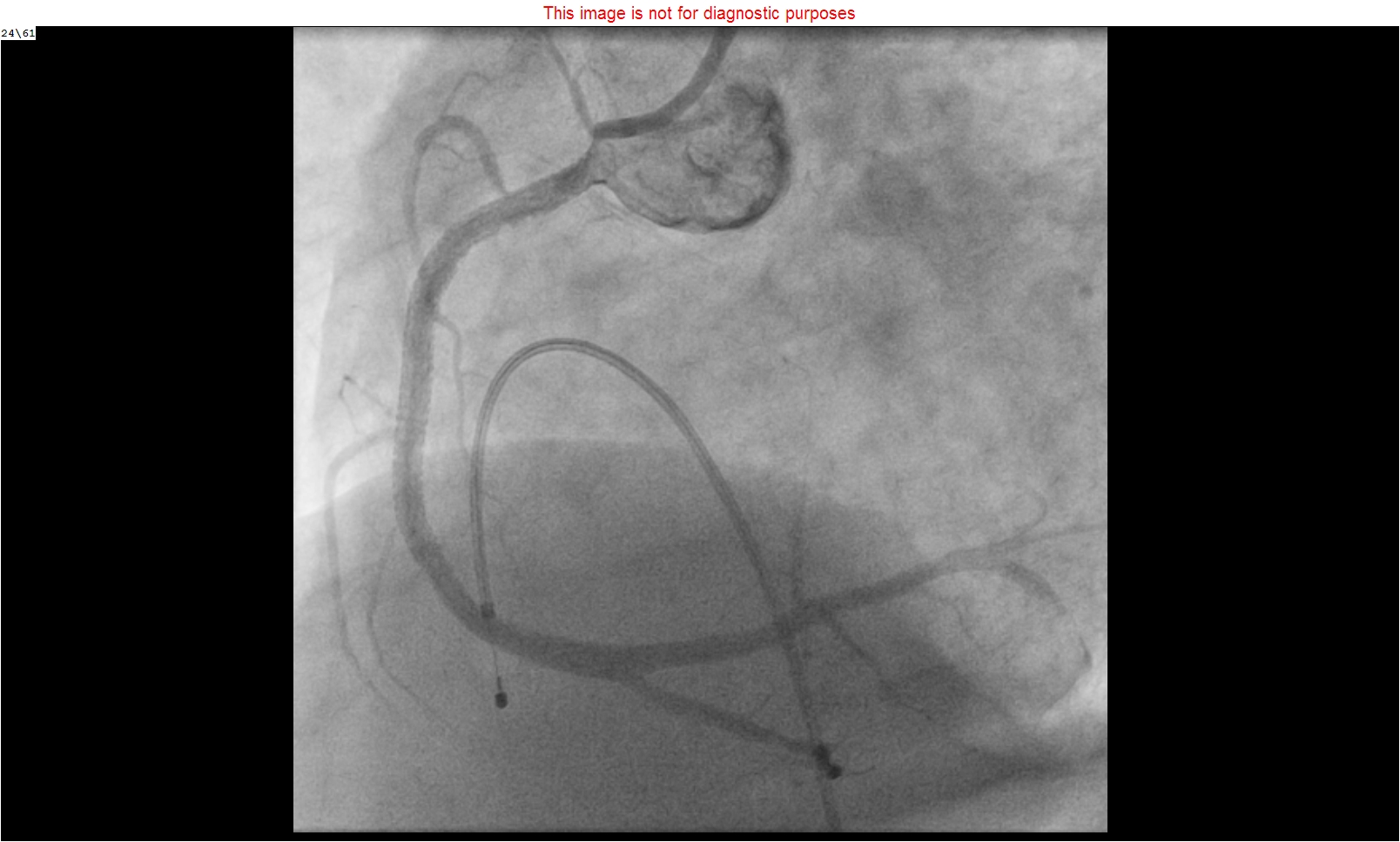
Relevant Catheterization Findings
The balloon-tipped temporary pacemaker implantation, through the right femoral vein, was done with satisfactory lead parameters. The coronary angiogram was done through the right femoral artery, which revealed 100% occlusion of proximal RCA with high thrombus load. The LAD was having a critical bifurcation lesion proximally. The LCx was non-dominant and had mild plaquing. Hence primary PCI to RCA and staged PCI to LAD was Planned
Interventional Management
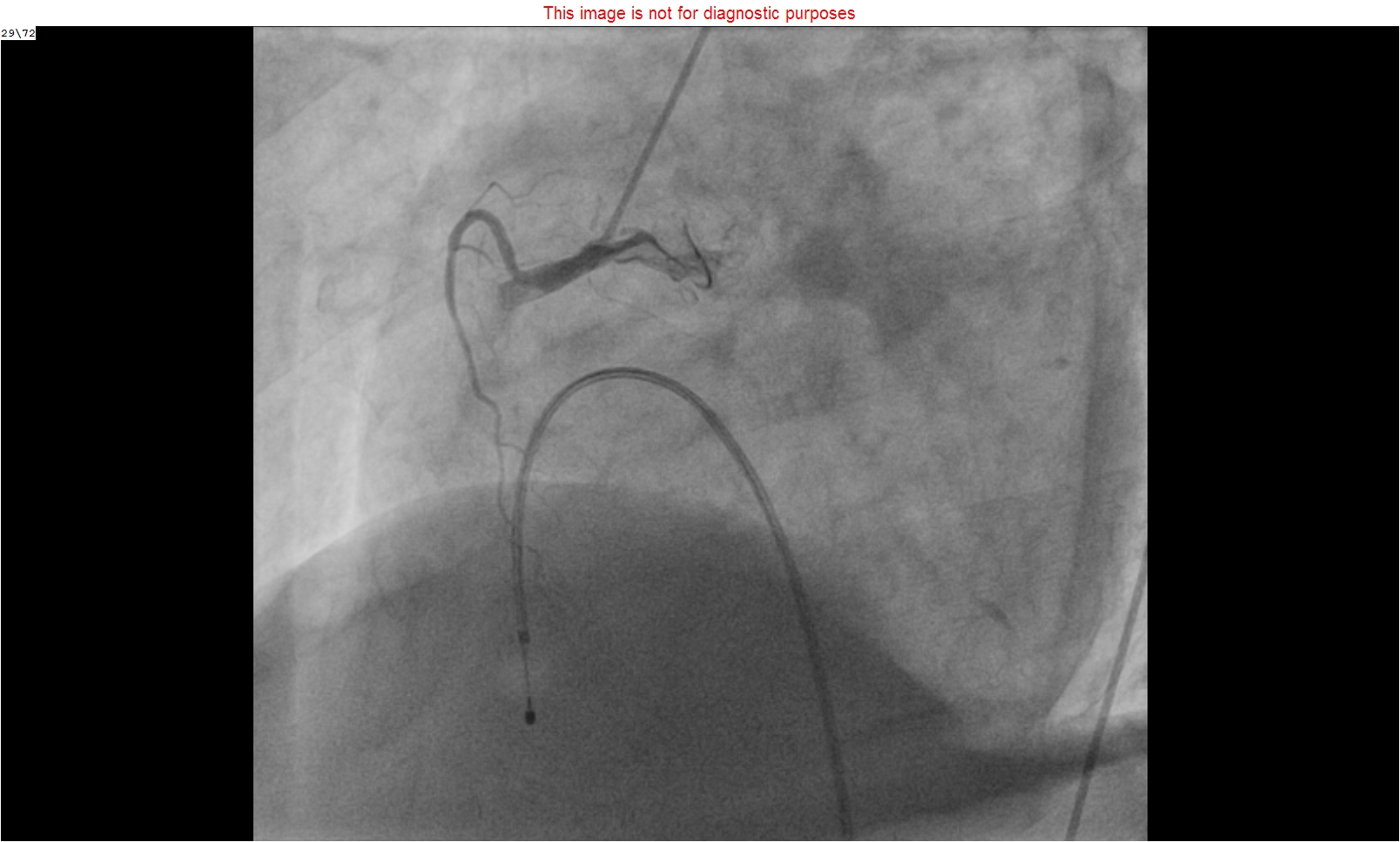
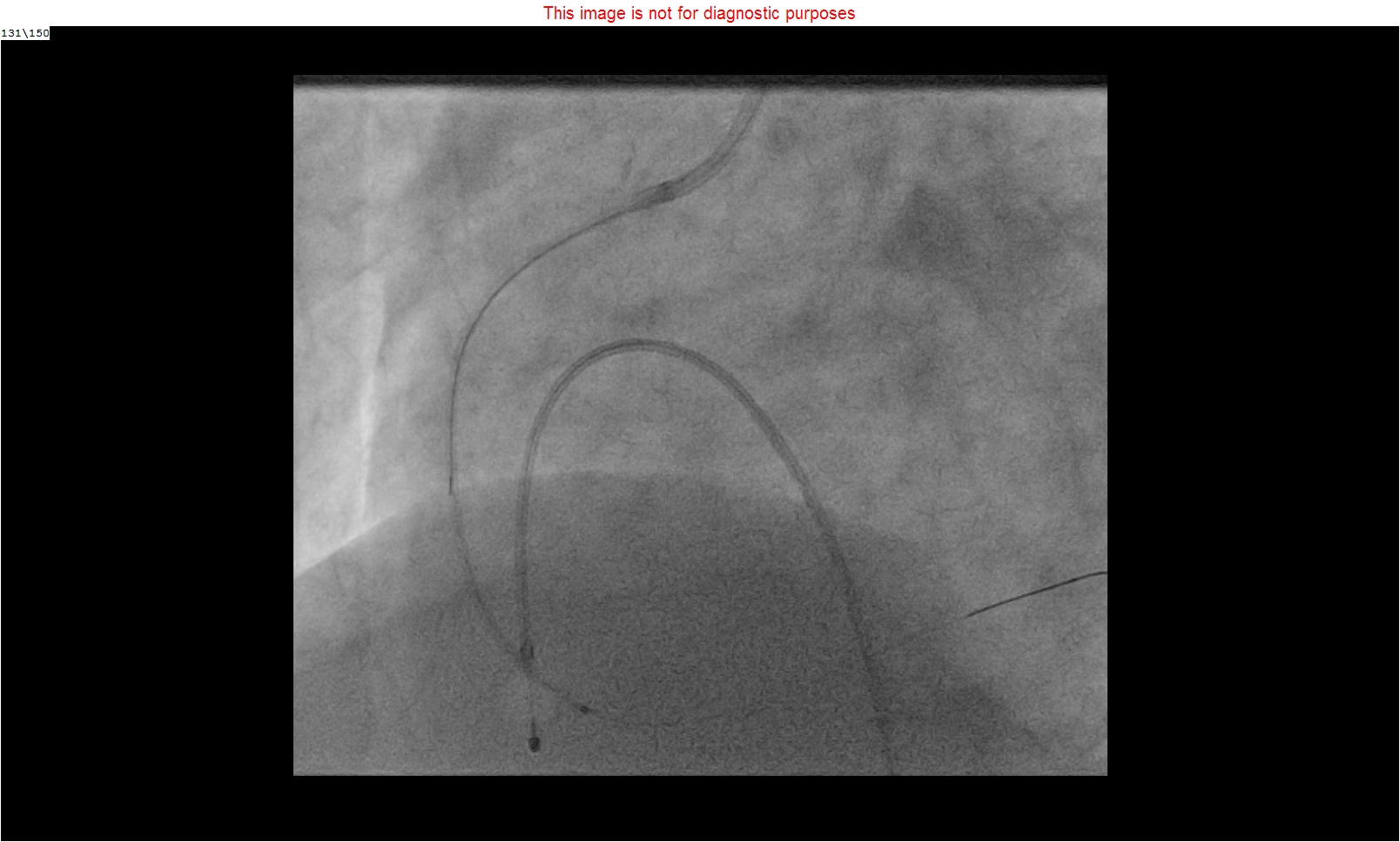
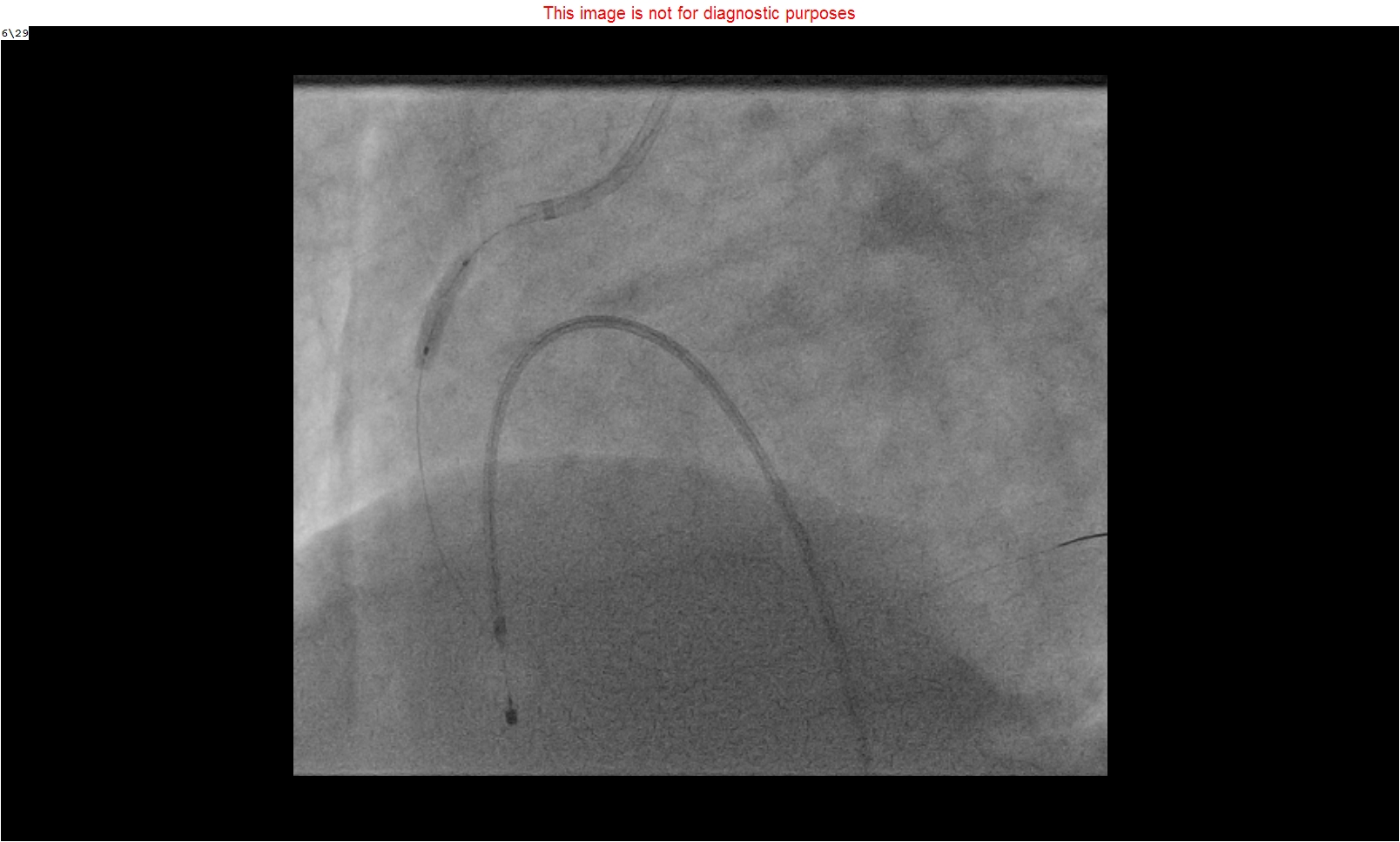
Procedural Step
For primary PCI to RCA, the Left main was hooked with JR 3.5, 7F’ guiding catheter. The lesion was crossed with the Sion blue guidewire. Considering the very high thrombus load, multiple attempts of thrombosuction were done with the help of Export 7F’ (Medtronic), and Eliminate 7F’ (Terumo) thrombus extraction catheters. Multiple pre-dilatations were done with 2 x 10 mm semi-compliant and 3 x 12 mm non-compliant balloons. Intracoronary abciximab, nicorandil, diltiazem and sodium nitroprusside were given at the distal coronary bed. Even after such exhaustive effort, the TIMI 3 flow could not be achieved and the thrombus burden was still very high. Hence the intracoronary thrombolysis was planned and it was done with the help of a “Fine Cross” microcatheter using streptokinase 5 lacs IU over half an hour. After that, the pre-dilatation was done with a 3.0 x 12 mm non-compliant balloon and then two overlapping drug-eluting stents (4 x 40 mm and 4 x 28 mm) were deployed. The post-dilatation was done with 4 x 28 mm same stent balloon at 18 atmospheric pressure with good end results and distal TIMI 3 flow. The patient was shifted to the coronary care unit for further management. His further hospital stay was uneventful and we could wean off the ventilator after 24 hours and was discharged after 4 days in stable condition.
Case Summary
High thrombus burden is always a cause of concern during primary PCI and affects the prognosis. If the thrombus burden still remains very high despite adequate pharmacological measures, multiple attempts of thrombosuctions and balloon dilatations, then the intra coronary thrombolysis can be done with great success.