
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-050
Physiology and Imaging Guided Non-left Main Bifurcation Percutaneous Coronary Intervention
By Seng Hsiung Toh, Zhen-Vin Lee
Presenter
Seng Hsiung Toh
Authors
Seng Hsiung Toh1, Zhen-Vin Lee2
Affiliation
Queen Elizabeth II, Malaysia1, KPJ Damansara Specialist Hospital 2, Malaysia2,
View Study Report
TCTAP C-050
CORONARY - Bifurcation/Left Main Diseases and Intervention
Physiology and Imaging Guided Non-left Main Bifurcation Percutaneous Coronary Intervention
Seng Hsiung Toh1, Zhen-Vin Lee2
Queen Elizabeth II, Malaysia1, KPJ Damansara Specialist Hospital 2, Malaysia2,
Clinical Information
Patient initials or Identifier Number
AK
Relevant Clinical History and Physical Exam
60 year old lady with underlying hypertension, dyslipidemia, ischemic stroke, and osteoarthritis.Admitted in August 2022 for unstable angina.After reviewing computed tomography coronary angiogram, patient agreed for coronary intervention.Clinical examination showed no neurological deficits or signs of heart failure.
Relevant Test Results Prior to Catheterization
Hemoglobin 9.4 g/dL, Creatinine 54 umol/L, LDL 1.72 mmol/LElectrocardiogram sinus rhythm with no ST segment changes.Echocardiography showed preserved ejection fraction, no regional wall motion abnormalities or valve disease.
Relevant Catheterization Findings
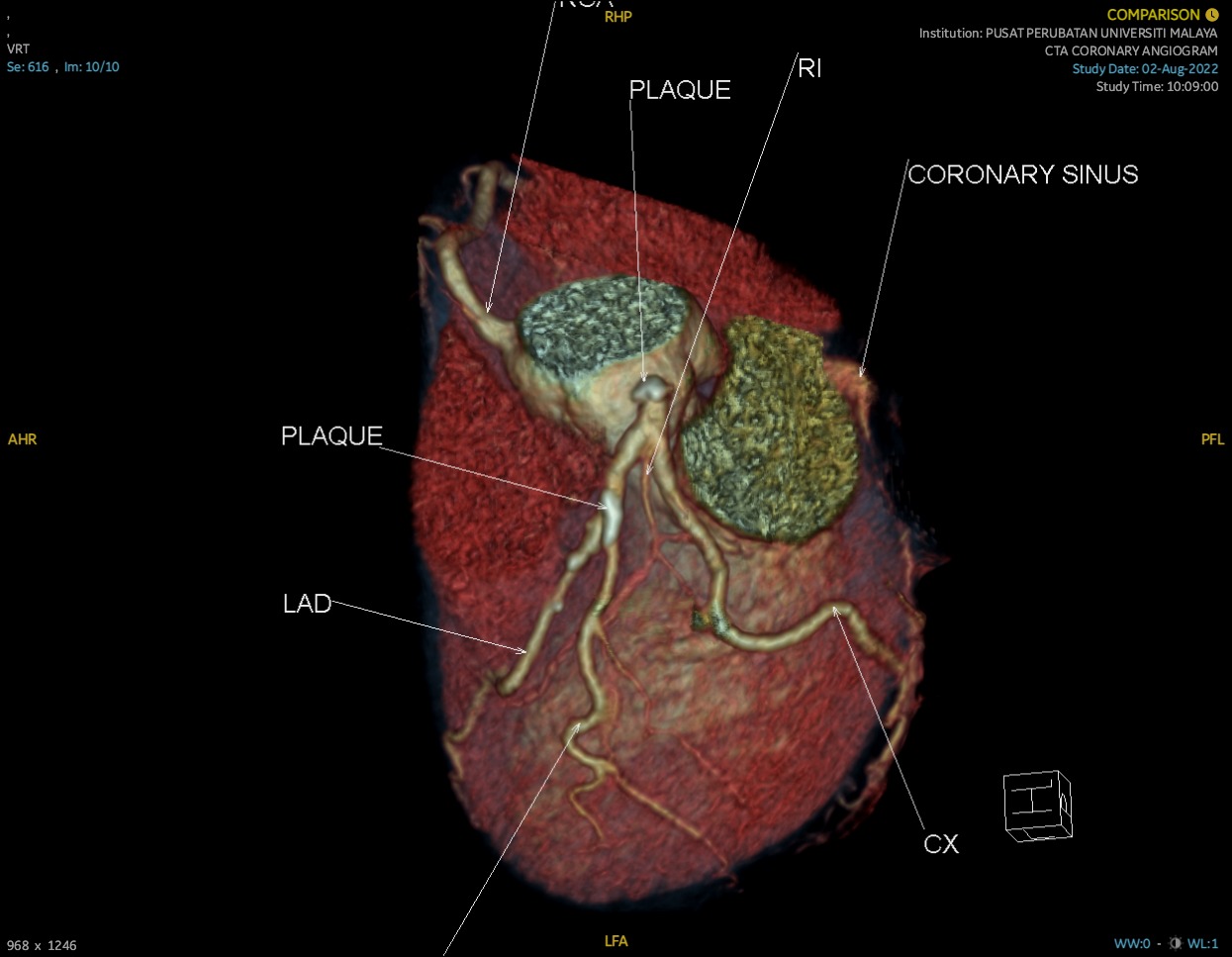
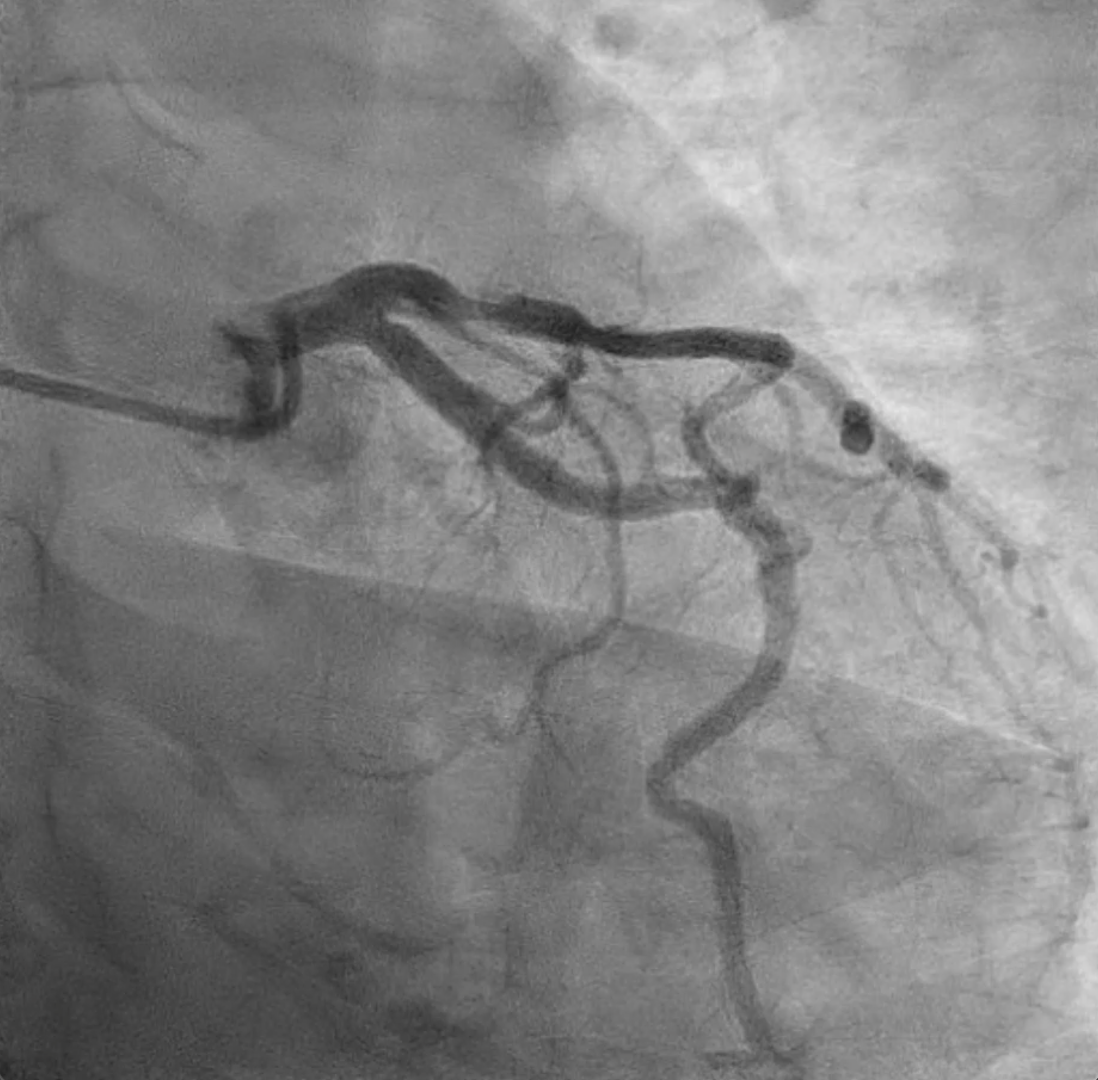
Mild to moderate calcification of left main and left anterior descending (LAD).Bifurcation lesion, Medina 0,1,1 involving proximal LAD and main diagonal. Eccentric plaque with stenosis 50-60% of proximal LAD and 50-70% stenosis of ostium to proximal segment of main diagonal. TIMI 3 flow.Left circumflex co-dominant, no significant lesion.Right coronary artery no significant lesion.


Interventional Management
Procedural Step
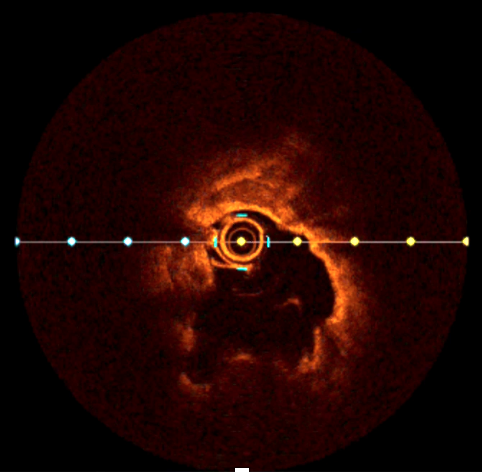
1. Diagnostic angiography with Terumo 5 French TIG showed moderate left anterior descending (LAD) calcification with mid segment eccentric plaque involving ostium to proximal segment of main diagonal, bifurcation 0,1,1.2. 6 French Cordis XB 3.0 guiding catheter engaged to left coronary artery.3. Fractional flow reserve (FFR) measurement of main diagonal and LAD with PressureWire X guidewire. Main diagonal 0.79 and LAD 0.78.4. Optical coherence tomography (OCT) assessment of lesions with Dragonfly Optis, noted superficial calcific plaque, more than 180 degree at bifurcation point with lipidic plaque at main diagonal and proximal LAD.5. Serial pre-dilatation of main diagonal and LAD with balloon Trek 2.5x12mm.6. Calcium modification of LAD with Scoreflex NC 3.0x15 mm.7. Drug eluting stent Xience Xpedition 3.5x38 mm deployed from ostium to mid segment LAD.8. Stent post-dilatation with NC Trek 3.5x15mm. Result TIMI 3 flow with no perforation or recoil.9. Side branch intervention with Mini Trek 1.5x12 mm, Prevail DCB 2.75x20mm unsuccessful.10. Post intervention FFR and OCT assessment performed.


Case Summary
1. Carina-tip angle and length, calcified and lipidic plaque are predictors of side branch compromise.2. Intra-coronary imaging enables optimisation of percutaneous intervention reduces in-stent restenosis.3. Physiological assessment of intermediate lesion aids intervention decision.4. Increment in post intervention FFR reduces future target vessel failure and major cardiac events.