
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-015
Meatball on a Spaghetti : A Case of Giant Coronary Aneurysmal
By Samshol Sukahri, Imran Zainal Abidin
Presenter
Samshol Sukahri
Authors
Samshol Sukahri1, Imran Zainal Abidin1
Affiliation
University Malaya Medical Centre, Malaysia1,
View Study Report
TCTAP C-015
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Meatball on a Spaghetti : A Case of Giant Coronary Aneurysmal
Samshol Sukahri1, Imran Zainal Abidin1
University Malaya Medical Centre, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Mr MND
Relevant Clinical History and Physical Exam
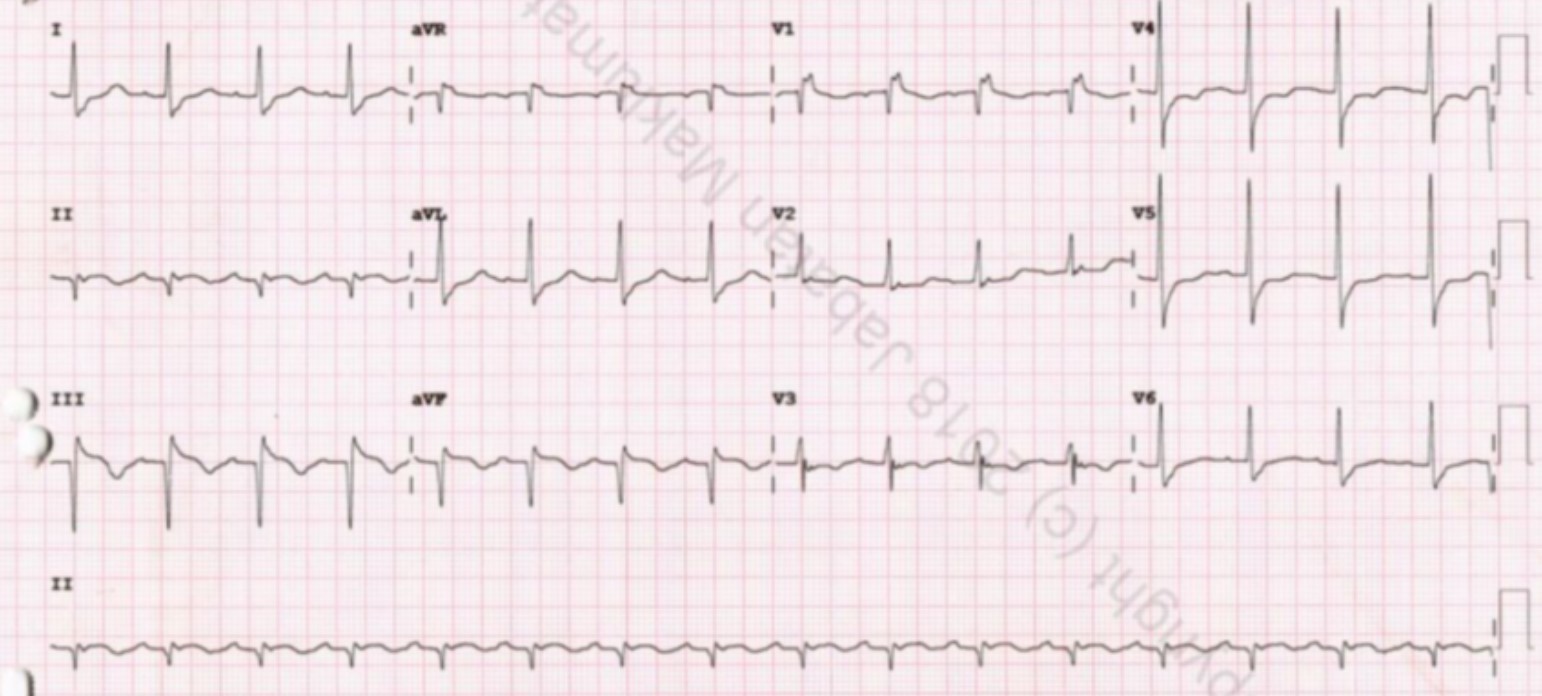
A 72-year-old gentleman underlying history of hypertension and dyslipidemia was electively admitted to the ophthalmology ward for eye surgery, unfortunately, developed acute typical chest pain. The physical findings were unremarkable and ECG noted the patient had an acute inferior myocardial infarction.
Relevant Test Results Prior to Catheterization
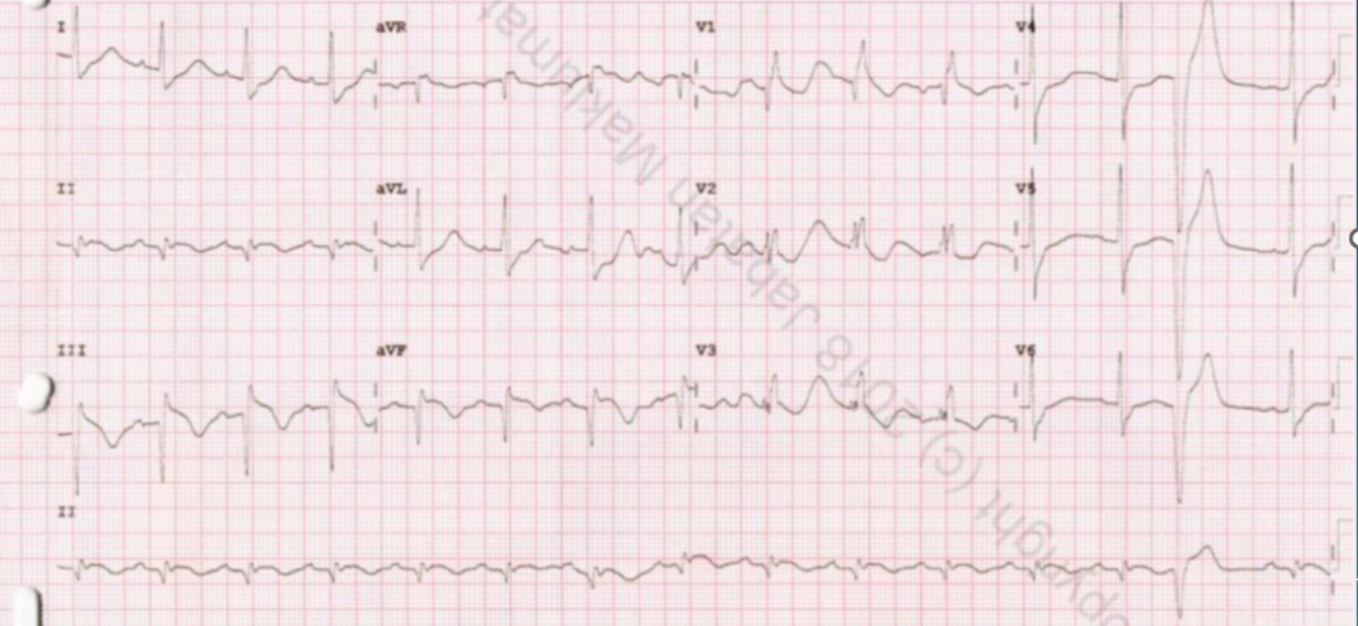
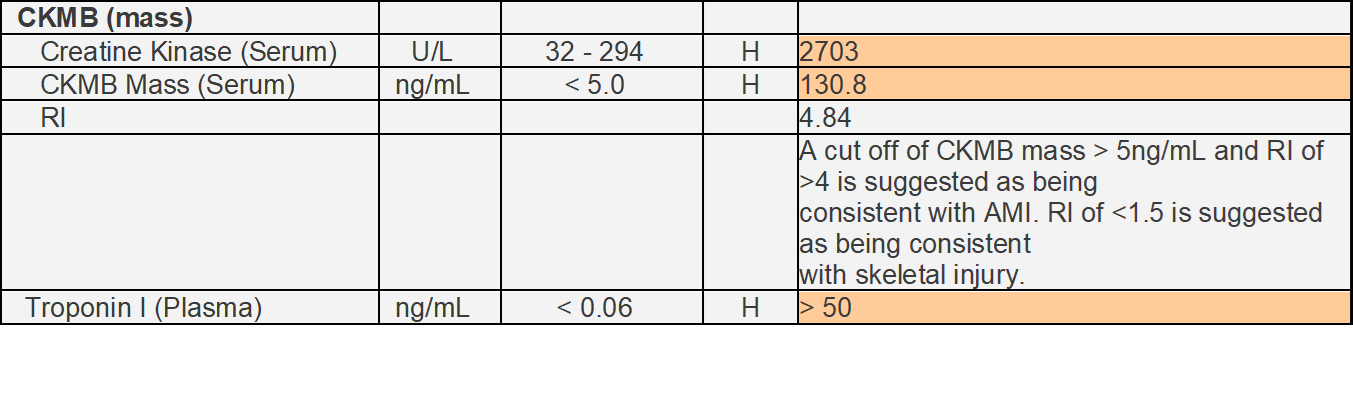
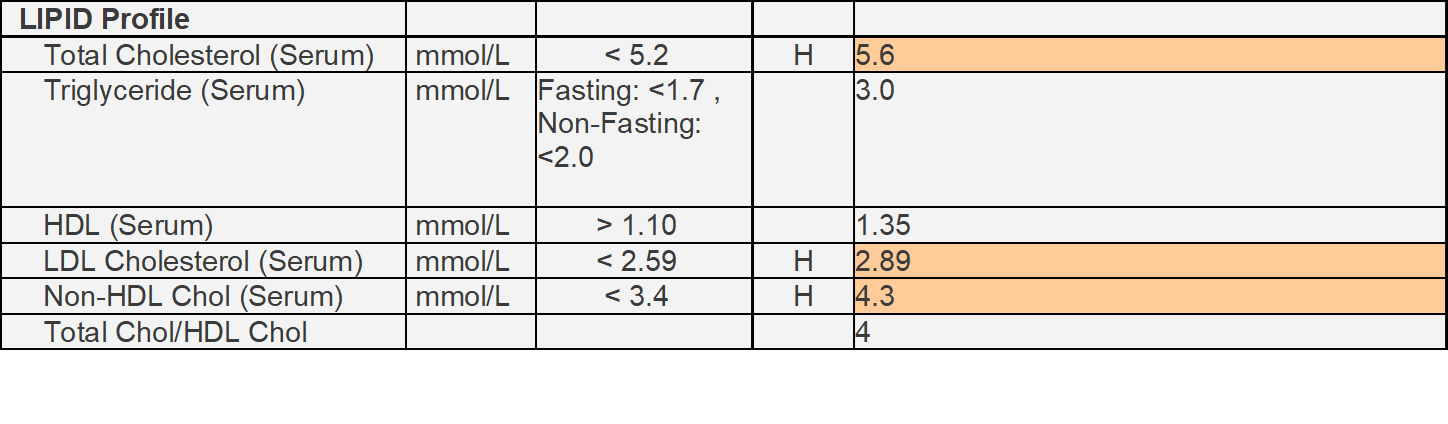
the ECG noted ST elevation over II, III, and AVL with RBBB over V1, V2, and V3 as well as PVCs. Cardiac enzymes were elevated, CK 2703 U/L, CK-MB 130.8 ng/mL, and Troponin I >50 ng/mL. the lipids profiles, LDL was 2.89 mmol/L
Relevant Catheterization Findings
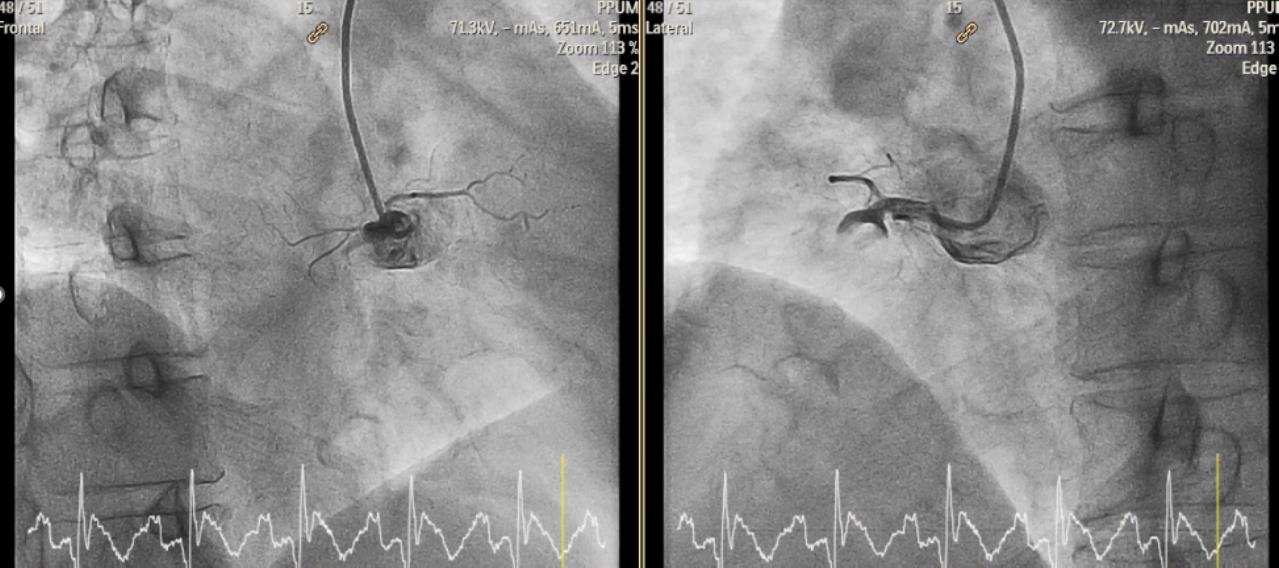
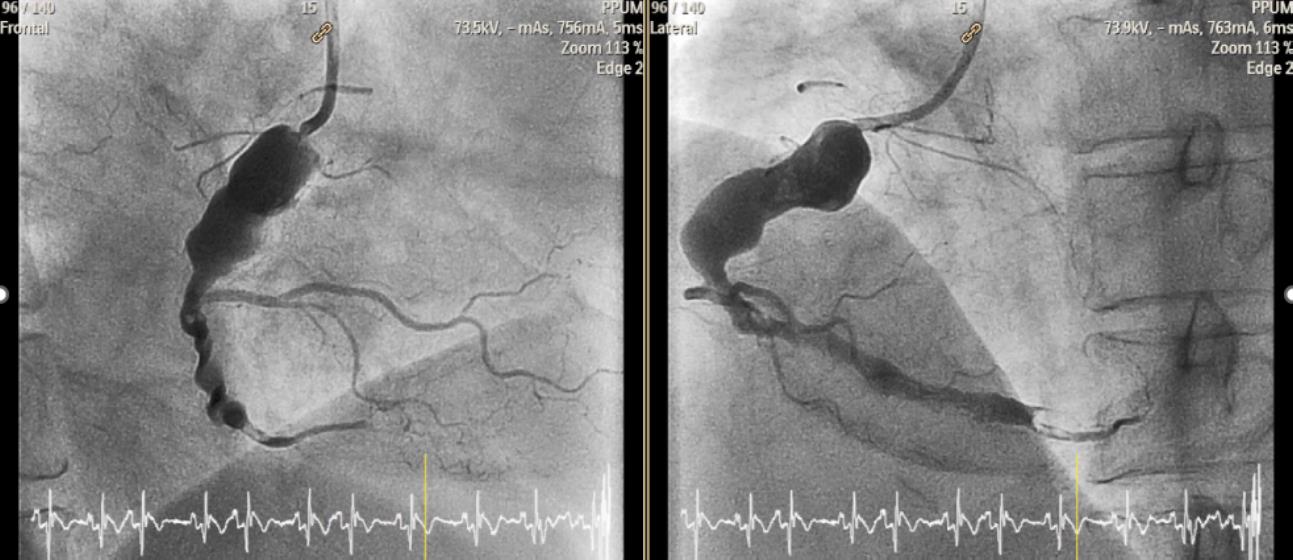
Thepatient underwent urgent primary PCI on the same day. 6F catheter was puncturedfrom the right radial artery. The diagnostic angiogram was performed noted ananeurysmal dilatation of proximal LAD and proximal LCX as well as huge aneurysmin proximal RCA (12mm) in which totally occluded RCA with huge thrombus burden
Interventional Management
Procedural Step
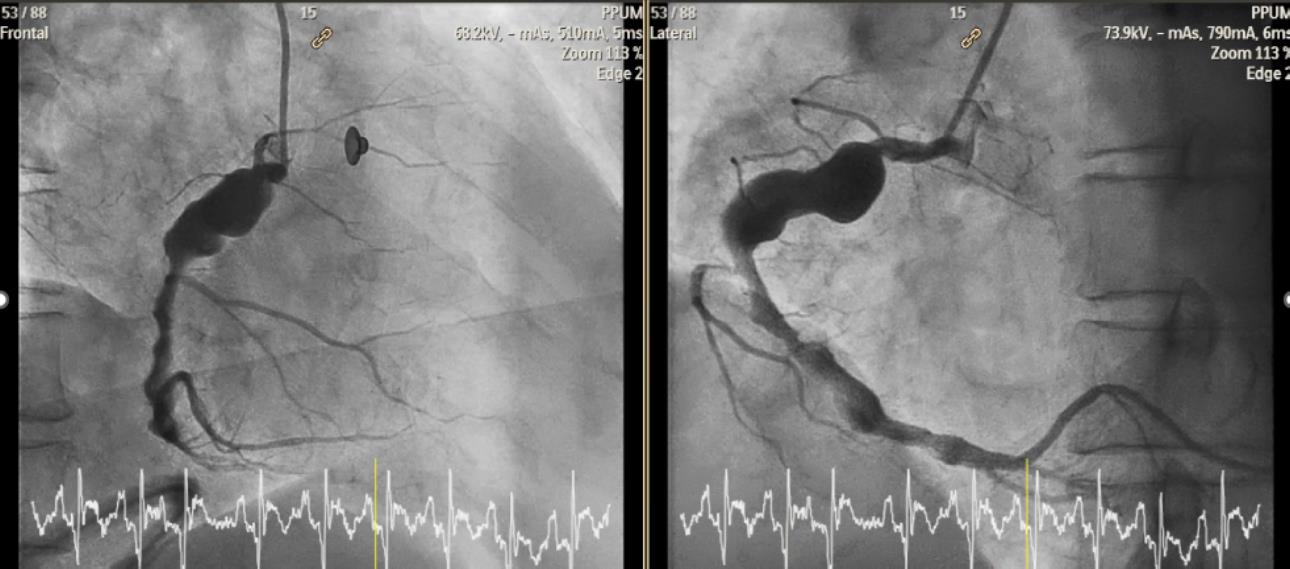
The 6F catheter was punctured from the right radial artery. The diagnostic angiogram was performed and noted an aneurysmal dilatation of proximal LAD and proximal LCX as well as a massive aneurysm in proximal RCA (12mm) which totally occluded RCA with a huge thrombus burden. Subsequently, JR 3.5 guide catheter was inserted and the Run-through floppy wire was passed through the acute total occlusion of RCA. The Thrombuster aspiration was performed, however still unable to establish the flow. Hence, intracoronary streptokinase 150,000 iu from the Thrombuster catheter was given immediately. TIMI II flow was established after intracoronary streptokinase. The vital signs were stable and ECG noted a resolution of ST elevation. The intravenous infusion of streptokinase 1,350,000 iu over 12 hours post-procedure. The relook angiogram was performed 5 days later and stated no residual thrombus with TIMI III flow in RCA. The patient was discharged well with a long-term plan for anticoagulants and aspirin.
Case Summary
Coronary Artery Ectasia (CAE) management should be tailored to individual patients depending on isolated CAE or CAE-concomitant obstructive coronary disease. CAE represents a form of atherosclerotic CAD, and aggressive risk factor modification for primary prevention using aspirin and statin is deemed necessary. Secondary prevention using anticoagulation is needed. However, never been examined in a large trial.