
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-082
Leave No Stone Unturned - Intervention to CTO of Anomalous RCA
By Abdul Ariff, Shaiful Azmi Yahaya
Presenter
Abdul Ariff
Authors
Abdul Ariff1, Shaiful Azmi Yahaya1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-082
CORONARY - Chronic Total Occlusion
Leave No Stone Unturned - Intervention to CTO of Anomalous RCA
Abdul Ariff1, Shaiful Azmi Yahaya1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
MSNK
Relevant Clinical History and Physical Exam
60 year old man, with background history of hypertension and dyslipidemia. He had NSTEMI in 2018, ECHO showed good EF of 56%. Coronary angiogram showed 2VD, with severe stenosis proximal LAD and CTO proximal RCA (anomalous origin from left SOV). As patient refused surgery, PCI to LAD was done, however, it was a failed attempt of PCI to CTO RCA. After 4 years, patient had worsening angina and ischemic study confirmed presence of large ischemia at RCA territory.

Relevant Test Results Prior to Catheterization
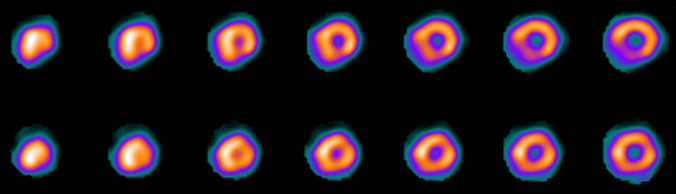
Gamma Nuclear Cardiology:There is a large area of stress induced ischemia in the LCX/RCA territory.The global left ventricular function is good.
Transthoracic Echo:EF 60%. TAPSE 1.9 cm. Mild aortic regurgitation. Normal left ventricular size.
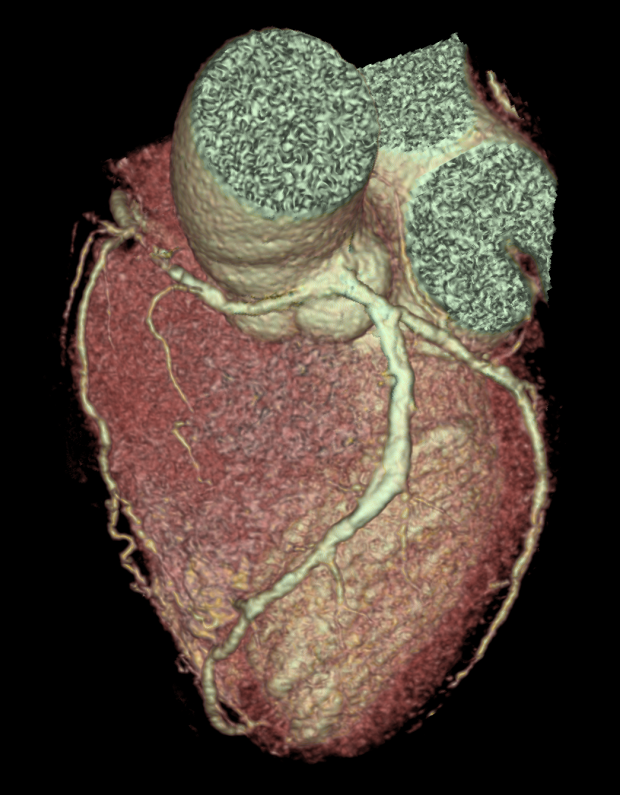
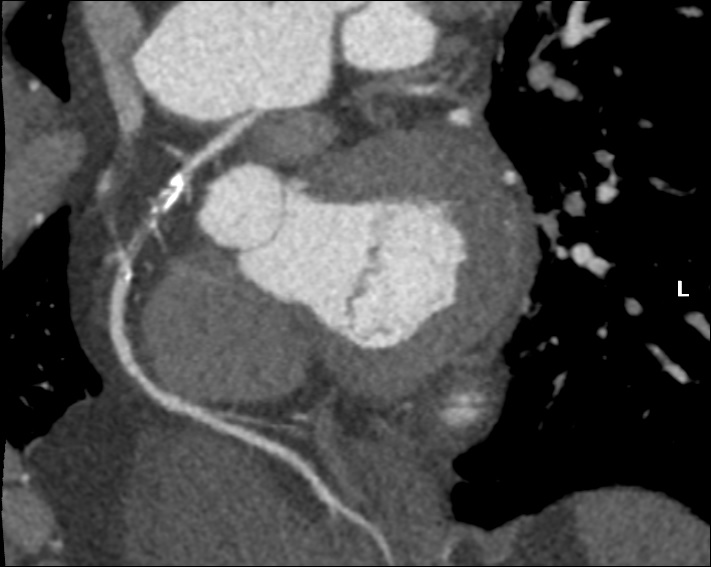
CT Cardiac:Anomalous origin of the ostial of the RCA from the border of the LCC and RCC with inter-arterial route. The ostial of the RCA has slit-like appearance. There is calcified plaque causing total occlusion at the proximal and mid RCA.
Transthoracic Echo:EF 60%. TAPSE 1.9 cm. Mild aortic regurgitation. Normal left ventricular size.
CT Cardiac:Anomalous origin of the ostial of the RCA from the border of the LCC and RCC with inter-arterial route. The ostial of the RCA has slit-like appearance. There is calcified plaque causing total occlusion at the proximal and mid RCA.
Relevant Catheterization Findings
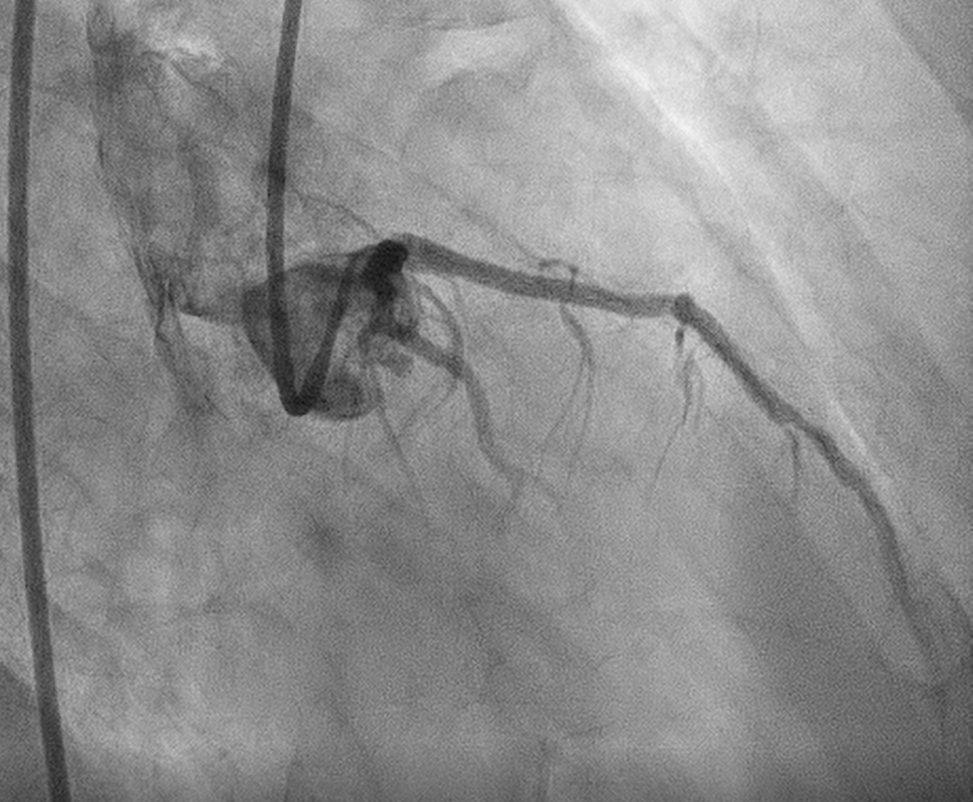
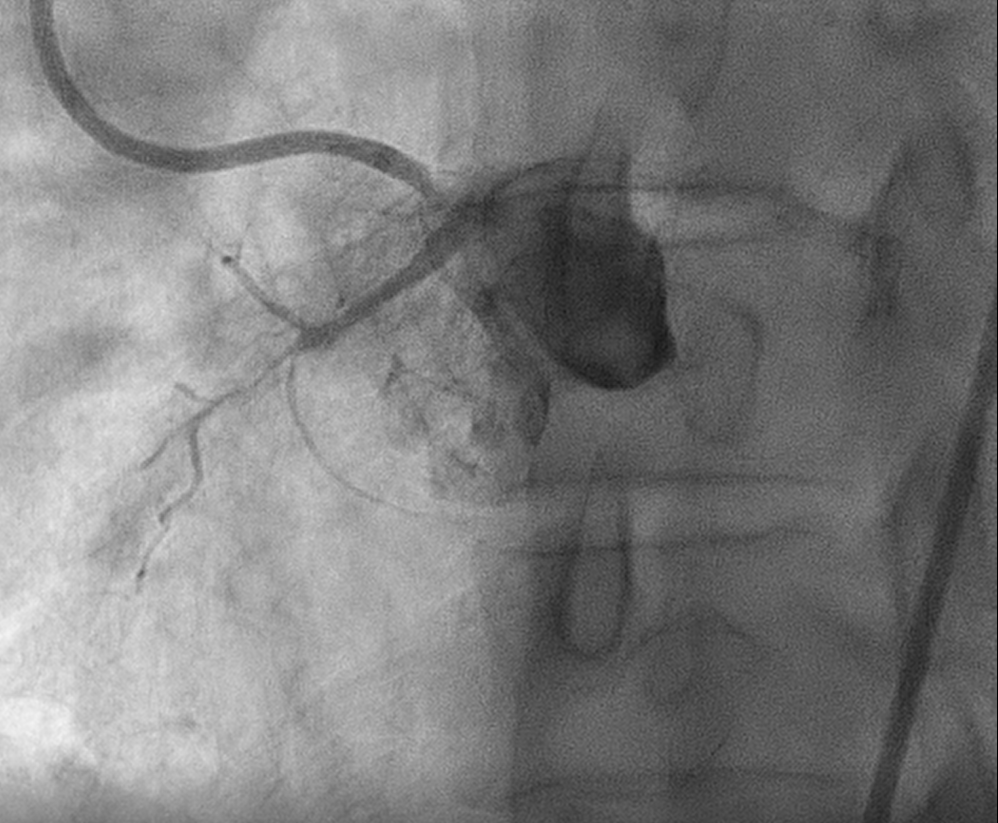
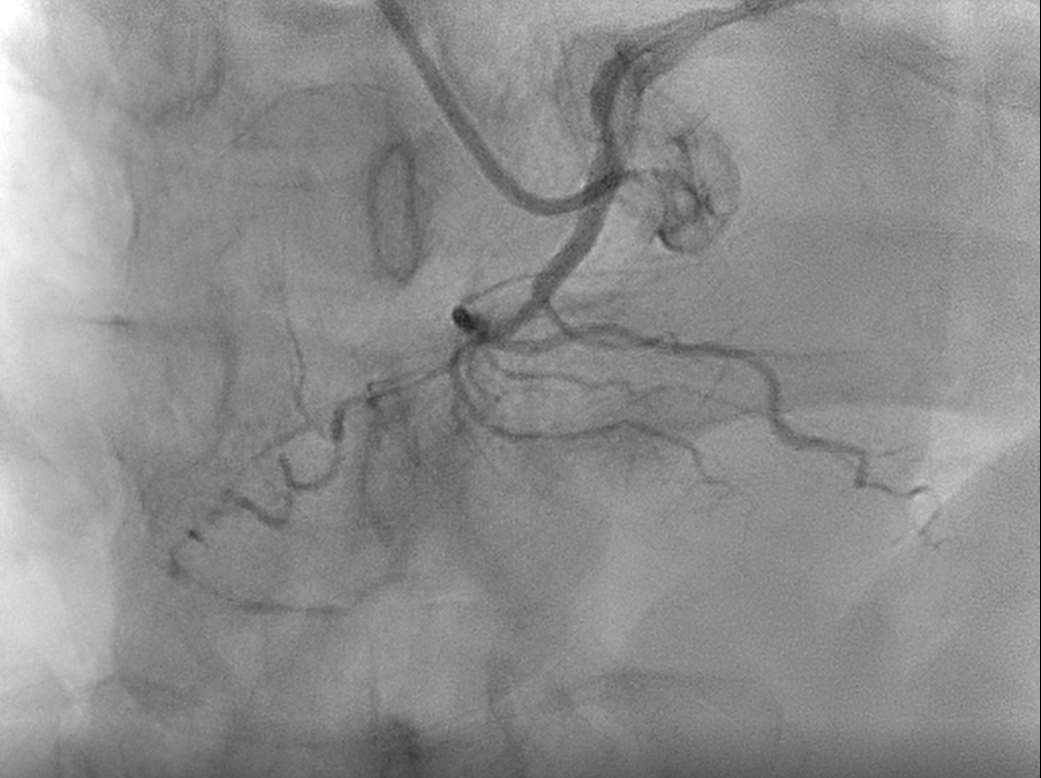
Left Main Stem : SmoothLeft Anterior Descending : Patent Left Anterior Descending stent, collaterals to Right Coronary ArteryLeft Circumflex Artery : Mild disease distallyRight Coronary Artery : Anomalous origin from left sinus of Valsalva, just slightly inferior and medial to origin of left main stem. Chronic Total Occlusion proximal Right Coronary Artery

Interventional Management
Procedural Step
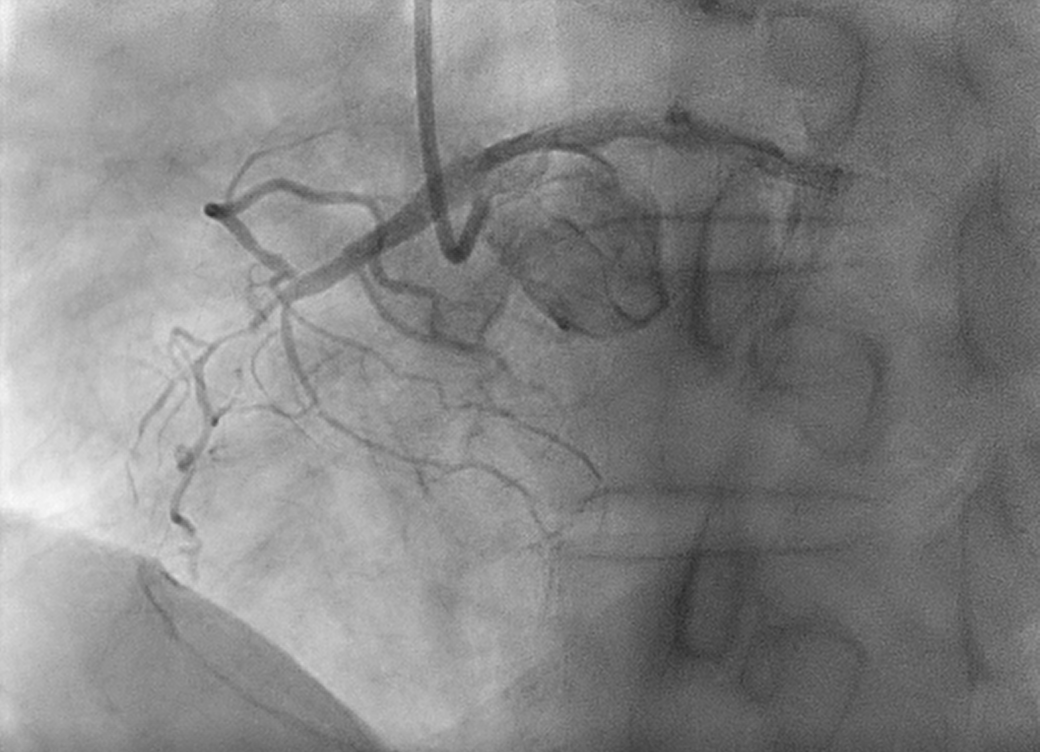
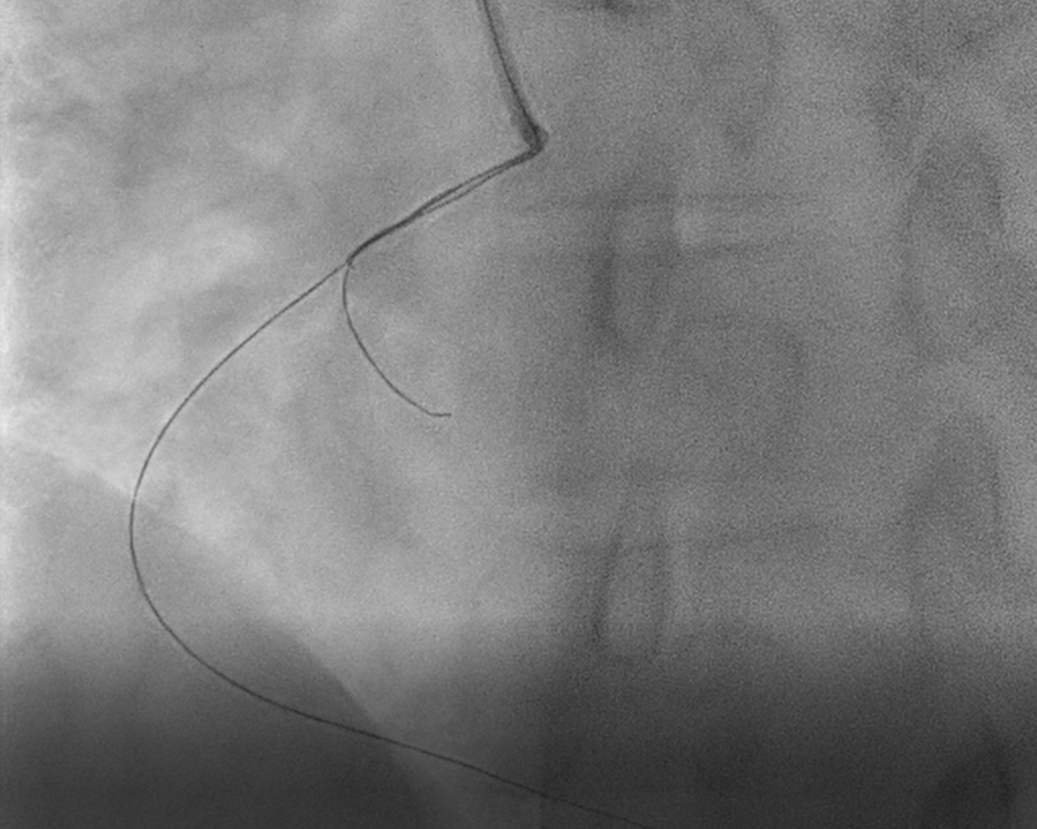
An attempt by intervention team 4 years ago was unsuccessful in view of failed selective engagement despite on 4 different catheters (JR 4, EBU 3.5, AL 0.75, AL 1.5). We’re comfortable with radial approach & unconventionally opted for JR 3.5 specifically to avoid injury to slit-like ostium & nearby left main. Engagement was difficult as JR kept on hugging the aortic wall. It was later made possible with “No-Touch” technique with gap created by Teflon, and wired successfully from outside. No backup force was expected from catheter throughout procedure. With Fielder XT as workhorse wire & Fielder FC in AV node branch for support, CTO was successfully crossed. We were unable to pass Caravel down despite additional soft wire at SA node branch for extra support. Microcatheter was escalated to Turnpike LP and with the aid of balloon anchor (2.0mm) at SA node branch, microcatheter was sent down in rotational movement. Sequential pre-dilatation& delivery of 1st stent (3.0/35mm) were done with balloon anchor support. In view of possible ischemia to SA node (intermittent junctional bradycardia), balloon anchor was omitted & soft wire was used as buddy wire for delivery of 2nd stent. However, it was not successful. Hence, 2nd stent (3.5/38mm) was also delivered via balloon anchor strategy. Balloon anchor was then removed and as a wire with best shaft support, Grand Slam was used as buddy wire for delivery of post-dilatation balloon.


Case Summary
This describes a rare case of CTO proximal anomalous RCA, arises from left SOV, just slightly inferior and medial to the left main. The ostial is slit-like with inferior take-off, hence poses additional technical challenge. This is only the 5th reported case of successful intervention of CTO of anomalous RCA from left SOV, with antegrade wire escalation strategy. Tough catheter engagement was overcome with meticulous & skillful catheter manipulation. Improvisation of variety of techniques for hardware delivery ensure procedural success. Equally essential, adjacent left main which was left unharmed was the icing on the cake.