
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-119
Multiple Complications In One Case: How We Handle It
By Chiao Hsiang Chang, Cheng-Chung Cheng
Presenter
Chiao Hsiang Chang
Authors
Chiao Hsiang Chang1, Cheng-Chung Cheng1
Affiliation
Tri-Service General Hospital, Taiwan1,
View Study Report
TCTAP C-119
CORONARY - Complications (Coronary)
Multiple Complications In One Case: How We Handle It
Chiao Hsiang Chang1, Cheng-Chung Cheng1
Tri-Service General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Medical record number 2901296
Relevant Clinical History and Physical Exam
The patient is a 61-year-old man with history of DM, Hypyerlipidemia and NSTEMI with 3-vessel disease s/p PCI on 2016/04/08.He has habit of smoking 1.5PPD for more than 30 years. He suffered from exertional dyspnea in recent 2 months and visited to our outpatient clinic. Physical examination showed bilateral clear breathing sound, minimal systolic murmur over apex. No pitting edema or clubbing finger was noted.
Relevant Test Results Prior to Catheterization
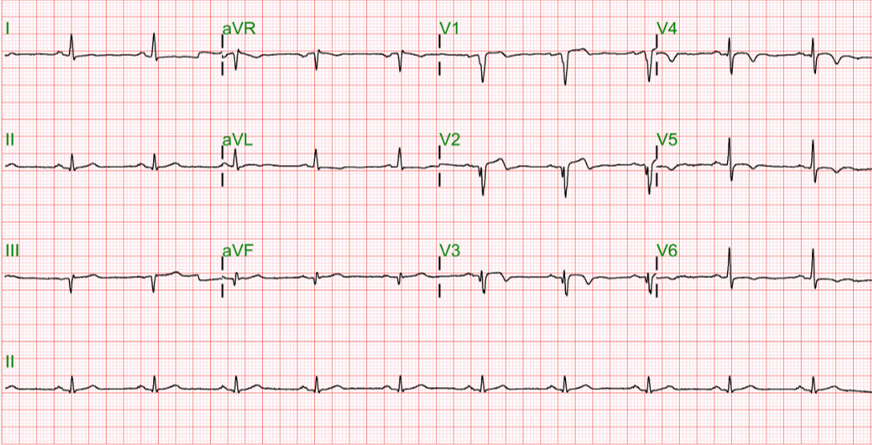
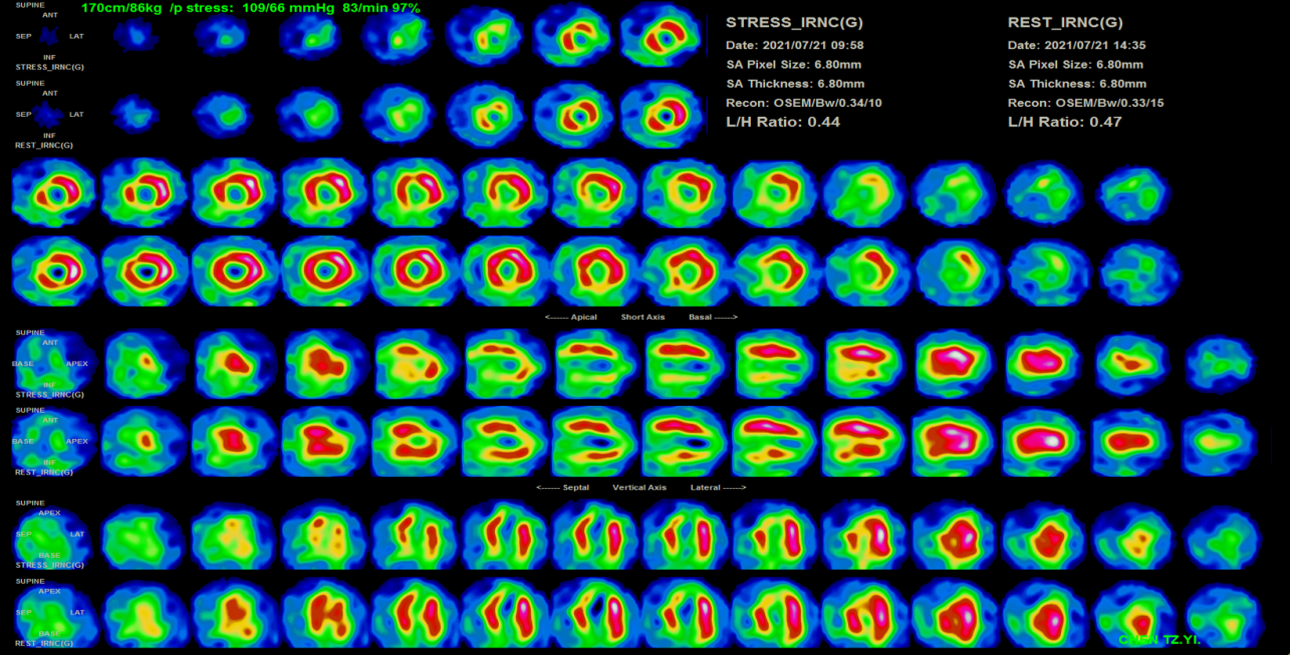
A series of examination was arranged for him. ECG showed QS pattern at lead III and biphasic T wave inversion at V1-3. Echocardiogram revealed left ventricle ejection fraction is 40-45%. Hypokinesia of apex and apical septum was noted. Tl-201 showed apicoanteriorwall, apex, posterolateral wall and inferior wall, measuring about 30% of LAD,20% LCx, and 80% of RCA territories.
Relevant Catheterization Findings
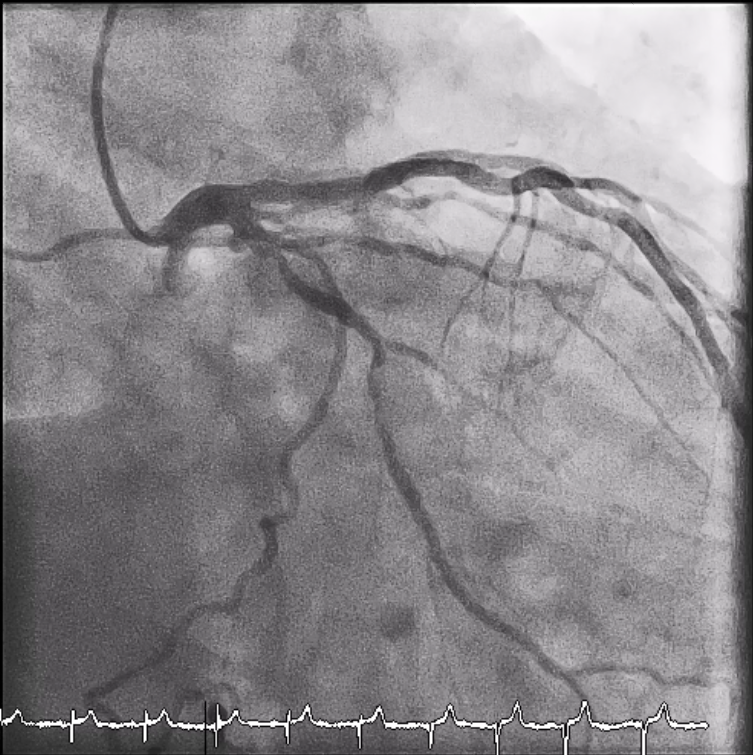
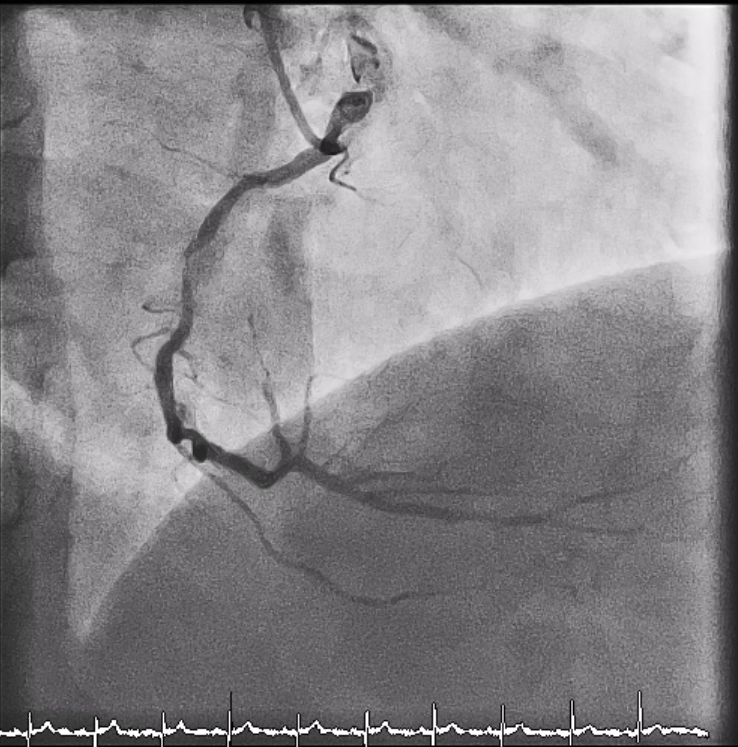
Coronaryangiogram revealed left anterior descending artery status post stenting withoutin stent restenosis. Left circumflex artery was severe stenosis andcalcification over proximal and middle portion and giving collateral to PL branch. Right coronary artery wassevere stenosis and calcification over proximal portion and total occlusionover PL with competing flow.

Interventional Management
Procedural Step
We used SAL1 6F to be our guiding catheter via radial artery and sion black wire was cross the lesion. Low-profile single marker compliant balloons tried to cross the lesion with Guideliner assist but the lesion was not dilatable. So we planned to used rotational atherectomy to prepare the lesion. First complication was happened that the burr out of the tract and vessel injury was noted. Secondary complication was floppy wire broken. We checked vital sign immediately and balloon inflated at injury site. No obvious tamponade sign and vital sign was stable. We kept the procedure but the low-profile single marker compliant balloons still failed to dilate the lesion. We changed the puncture site from radial artery to femoral artery to increase system stability. Rotational atherectomy was done again. This time, the lesion was successful to management.However, the third complication was happened. The 1.25 burr was entrapment. We used ST01 catheter to removed the burr successfully. The lesion was also predilated by non-compliant balloons and stenting with drug eluting stent. The broken wire was tried to removed by multiple wire method but failed. We used microsnare and removed the broken wire successfully. AAngiogram still showed proximal RCA perforation. Covered stent was stenting and no extravasation was found. failed


Case Summary
•Good guiding catheter engagement and good co-axial is important to all procedure and prevent catastrophic complication.