
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-144
Trouble Below: Spontaneous Internal Carotid Dissection
By Yuan-Kun Wu, Ying-Hsien Chen
Presenter
Yuan-Kun Wu
Authors
Yuan-Kun Wu1, Ying-Hsien Chen1
Affiliation
National Taiwan University Hospital, Taiwan1,
View Study Report
TCTAP C-144
ENDOVASCULAR - Carotid & Neurovascular Intervention
Trouble Below: Spontaneous Internal Carotid Dissection
Yuan-Kun Wu1, Ying-Hsien Chen1
National Taiwan University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
YPW
Relevant Clinical History and Physical Exam
A 54-year-old man with no known underlying condition reported sudden onset of hoarseness and dysphagia one day before the presentation at the emergency department. The neurological examination revealed uvula deviation to the right side and focal left-sided pharyngeal muscle weakness, compatible with CN IX/X palsy. The vital signs were as follows: blood pressure 142/95mmHg, pulse: 76/min, respiration: 18/min, temperature: 37'C. A nasogastric tube had to be placed for severe dysphagia.
Relevant Test Results Prior to Catheterization
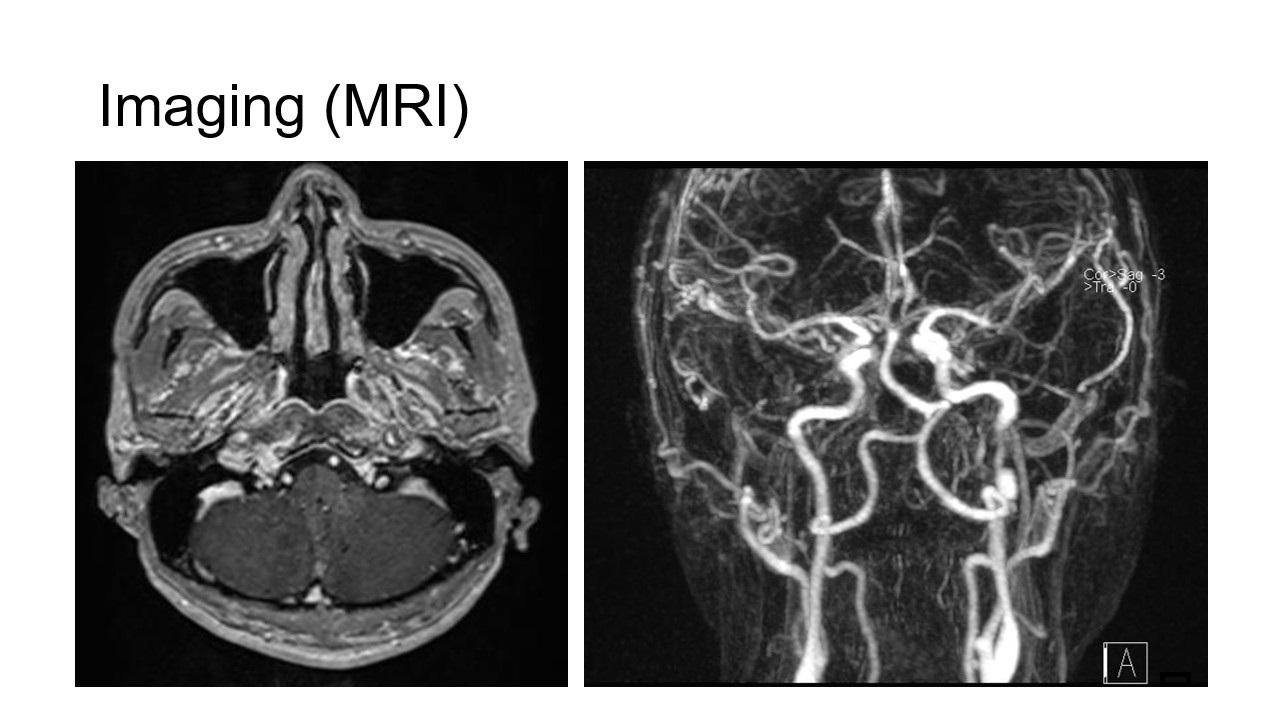
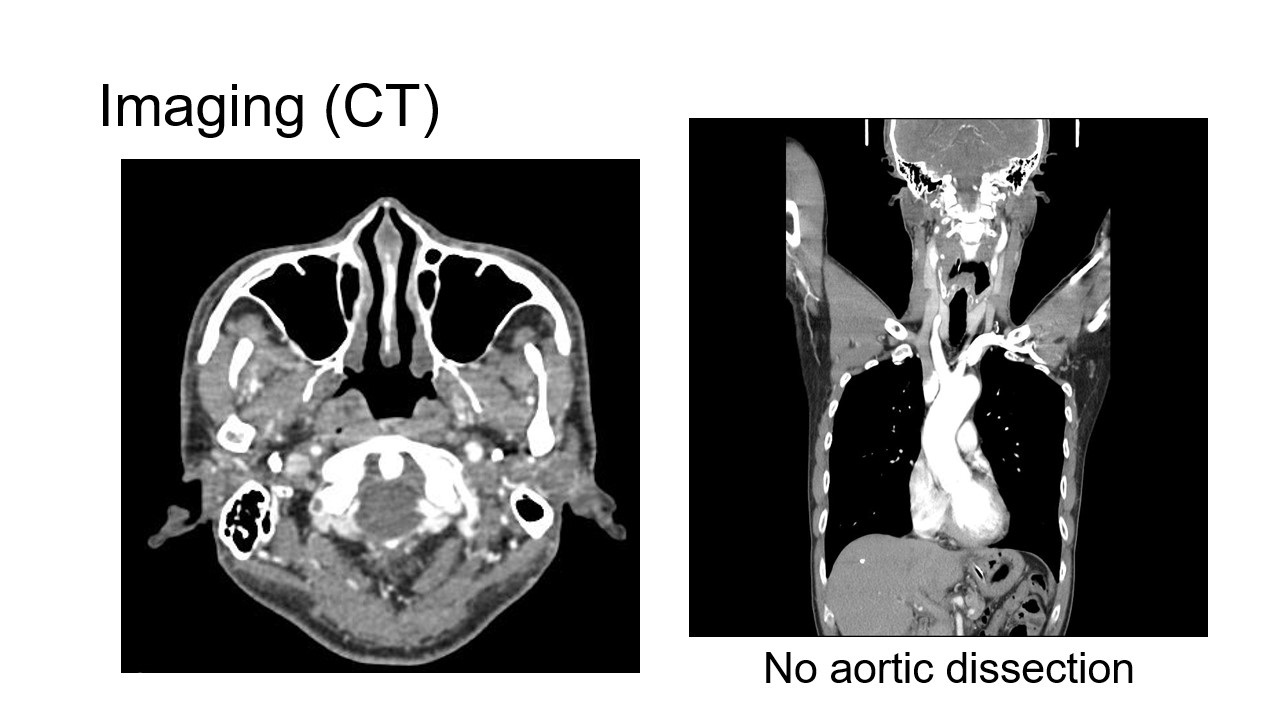
Under the tentative diagnosis of stroke, we arranged a brain magnetic resonance imaging (MRI). The imaging study did not reveal apparent signs of a recent stroke but indicated dissection of the left internal carotid artery with aneurysm formation over distal cervical segment (Figure 1). A computed tomography scan (CT) ruled out aortic dissection. The serological studies were negative for metabolic disorder and common risk factors for cardiovascular disease (Figure 2).
Relevant Catheterization Findings
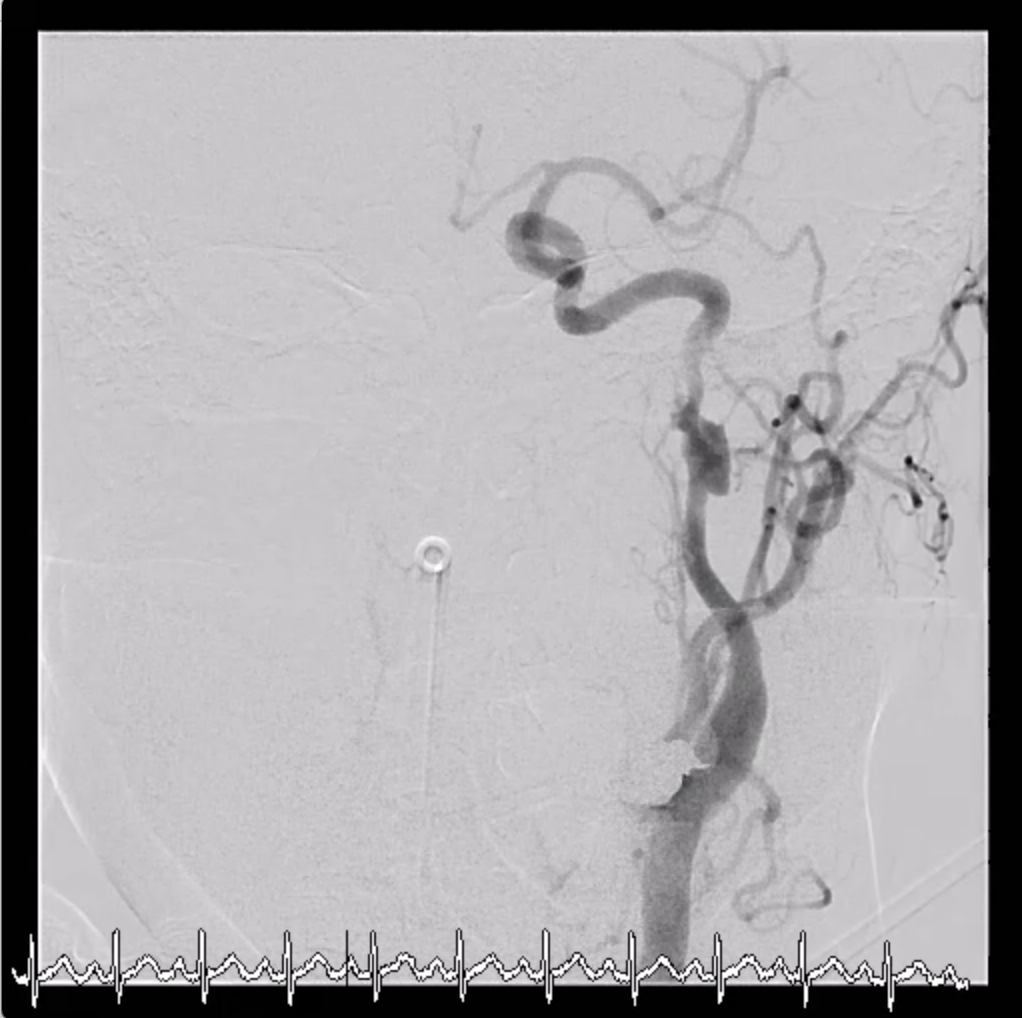
The patient agreed to endovascular intervention. All extracranial vessels were patent under standard angiography examination except for the left internal carotid artery. Dissection of the left internal carotid artery was noted from the cervical up to the petrous segment. An 11mm aneurysm was noted at the distal part of the cervical part of left internal carotid artery (Figure 1 and 2).

Interventional Management
Procedural Step
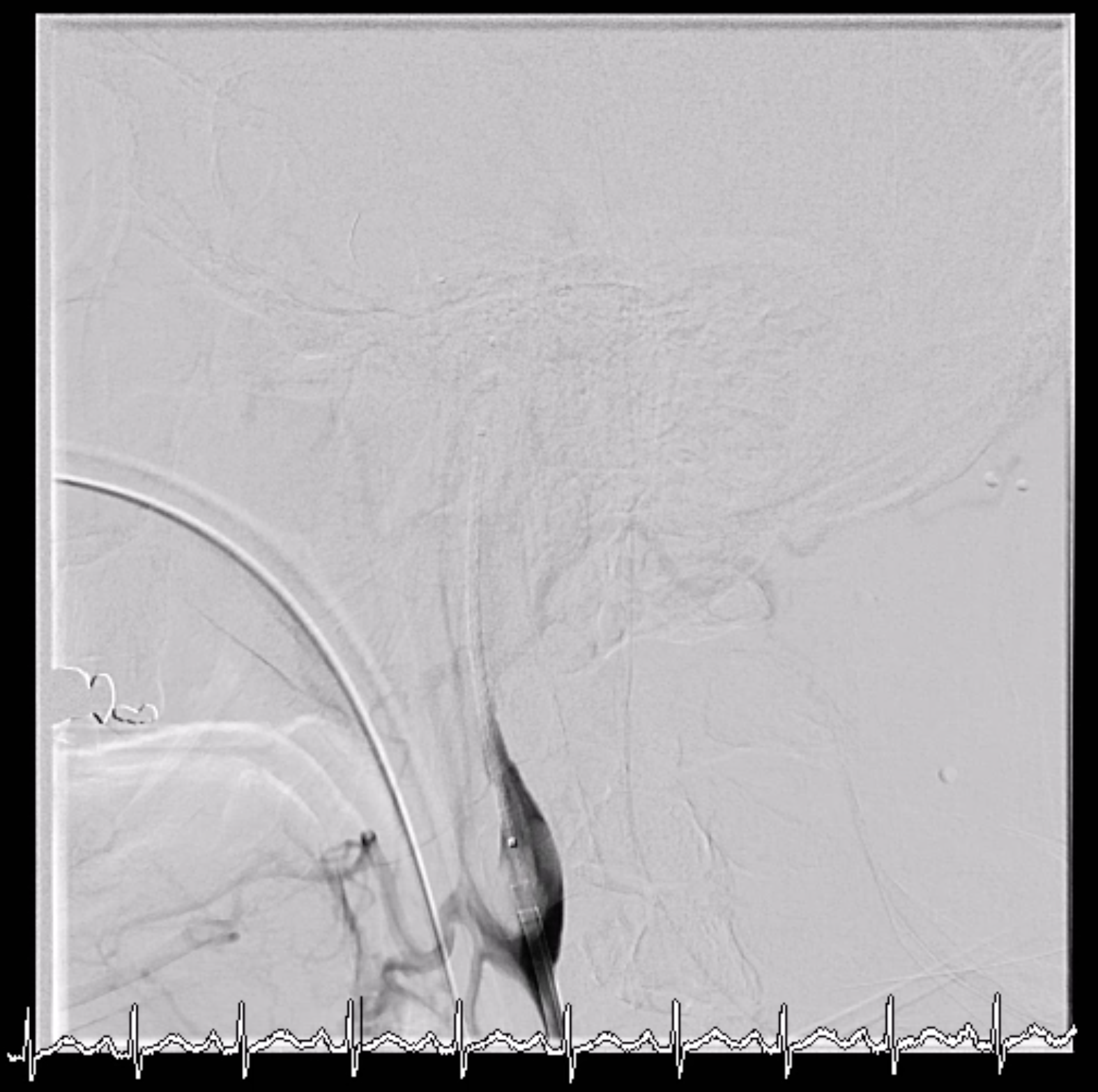
Treatment strategy was to place a cover stent over the aneurysm. A femoral approach was selected with an 8Fr JR guiding catheter engaged to the left common carotid artery. Initial wiring crossed the dissection section with Asahi Sion wire with a Terumo Finecross microcatheter. Successful wiring was achieved. The distal lumen was confirmed with tip injection. The microcatheter was then removed by balloon trapping technique with Boston Emerge (2.5mm x 15 mm) semi-compliant balloon. Over the Sion wire, we delivered ev3 SpiderFx Embolic Protection Device (5mm) in the distal petrous segment of the carotid artery, more distal than we commonly would for carotid procedures. Over the SpiderFx wire, we deployed the Viabahn Endoprosthesis (5 x 50mm) (Figure 1). No reflow of the carotid artery was noted after stent placement; at this stage, the patient reported intolerable left-sided headache. Balloon angioplasty was performed on the proximal petrous portion, and flow was restored. Angiography still showed a leak into the dissection cavity (Figure 2). We, therefore, placed an Abbott Graftmaster (3.5mm x 19 mm). The final flow of the left internal carotid was restored (Figure 3).


Case Summary
Spontaneous internal carotid dissection accounts to less than 2% of ischemic strokes. These patients are often presented with stroke-like symptoms. Endovascular therapy remains a viable treatment option and may potentially restore brain perfusion resulting in more promising outcome. However, further studies are required to confirm the outcome of this treatment option.