
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-198
All Roads Lead to Rome
By Kar Lok Leo Lai, Kevin Ka-Ho Kam, Sylvia SW Au, Ka Lung Chui, Randolph Hung-Leung Wong, Alex, Pui Wai Lee, Bryan Ping-Yen Yan, Eugene Brian Wu, Joseph YS Chan, Kent, Chak Yu So
Presenter
Kar Lok Leo Lai
Authors
Kar Lok Leo Lai1, Kevin Ka-Ho Kam1, Sylvia SW Au1, Ka Lung Chui1, Randolph Hung-Leung Wong1, Alex, Pui Wai Lee1, Bryan Ping-Yen Yan2, Eugene Brian Wu1, Joseph YS Chan1, Kent, Chak Yu So3
Affiliation
Prince of Wales Hospital, Hong Kong, China1, The Chinese University of Hong Kong, Hong Kong, China2, Prince Of Wales Hospital, Chinese University of Hong Kong, Hong Kong, China3,
View Study Report
TCTAP C-198
STRUCTURAL HEART DISEASE - Valvular Intervention: Aortic
All Roads Lead to Rome
Kar Lok Leo Lai1, Kevin Ka-Ho Kam1, Sylvia SW Au1, Ka Lung Chui1, Randolph Hung-Leung Wong1, Alex, Pui Wai Lee1, Bryan Ping-Yen Yan2, Eugene Brian Wu1, Joseph YS Chan1, Kent, Chak Yu So3
Prince of Wales Hospital, Hong Kong, China1, The Chinese University of Hong Kong, Hong Kong, China2, Prince Of Wales Hospital, Chinese University of Hong Kong, Hong Kong, China3,
Clinical Information
Patient initials or Identifier Number
MCH
Relevant Clinical History and Physical Exam
An 82-year-old gentleman presented with symptomatic severe aortic stenosis with recurrent dizziness and angina. He also had exertional dyspnea with new onset leg oedema (New York Heart Association Class III). His past medical history included severe COPD (FEV1 16%, FVC 22%). His blood pressure was 132/64 mmHg and a heart rate of 52 bpm. His respiratory rate was 16 with oxygen saturation of 98% on room air. His Katz index was 6, Chinese Lawton of 25/27 and 5 minutes walking test of 7.15 seconds.
Relevant Test Results Prior to Catheterization
His laboratory tests showed hemoglobin of 14 g/dL, platelet of 151 x 10^9/l, creatinine of 89 umol/L and albumin of 38 g/L. His baseline electrocardiogram showed sinus rhythm with right bundle branch block. His echocardiogram demonstrated left ventricular systolic function of 54%, the mean trans-aortic gradient of 46mmHg, and an aortic area of 0.6cm^2. There were mild aortic and mitral regurgitations only.
Relevant Catheterization Findings
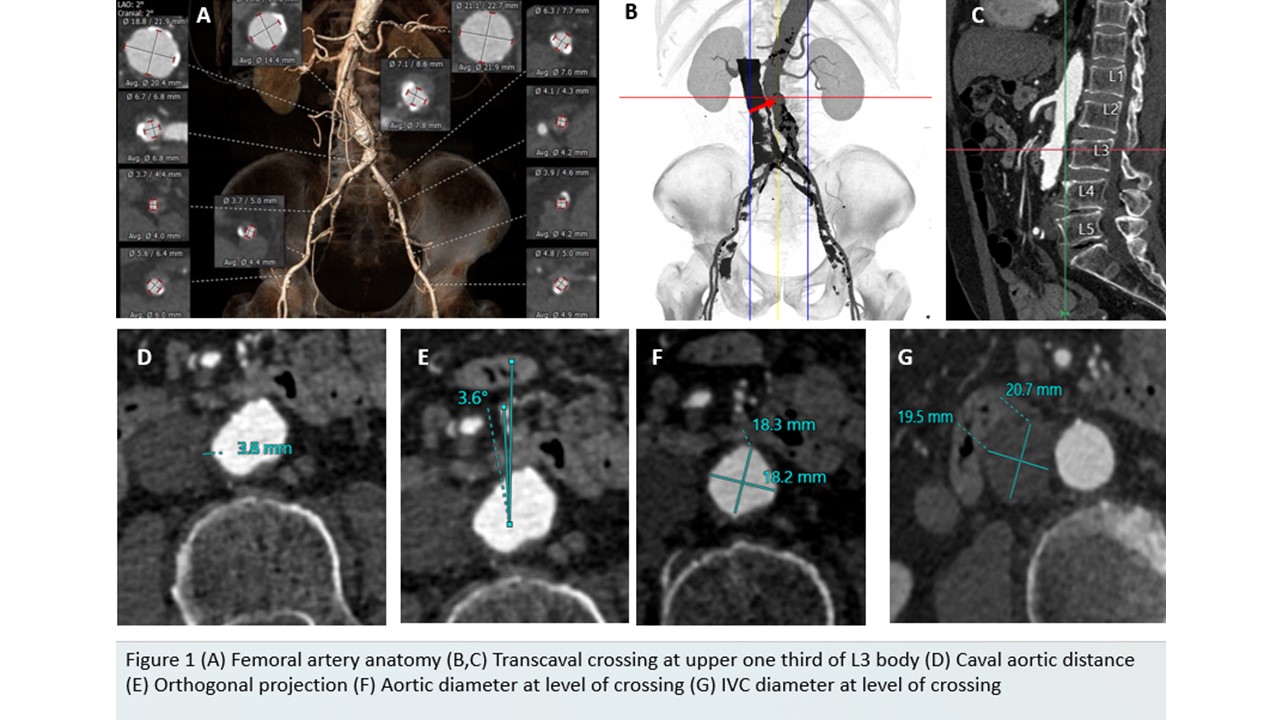
He underwent coronary angiogram and showed proximal to mid left anterior descending (LAD) lesion of 70%, other coronary arteries did not show any significant stenosis. His computed tomography (CT) revealed small bilateral femoral arteries, axillary and subclavian arteries were also too small. Trans-carotid or direct aortic routes were potentially feasible. However, his CT cerebral angiogram showed incomplete Circle of Willis. His Society of Thoracic Surgeons' mortality risk score was 5.6%.
Interventional Management
Procedural Step
In view of elevated risk of cerebral ischaemia for transcarotid TAVI, and high risk of direct aortic access (poor lung function), Heart team recommended transcaval TAVI as the preferred alternative access for this patient.
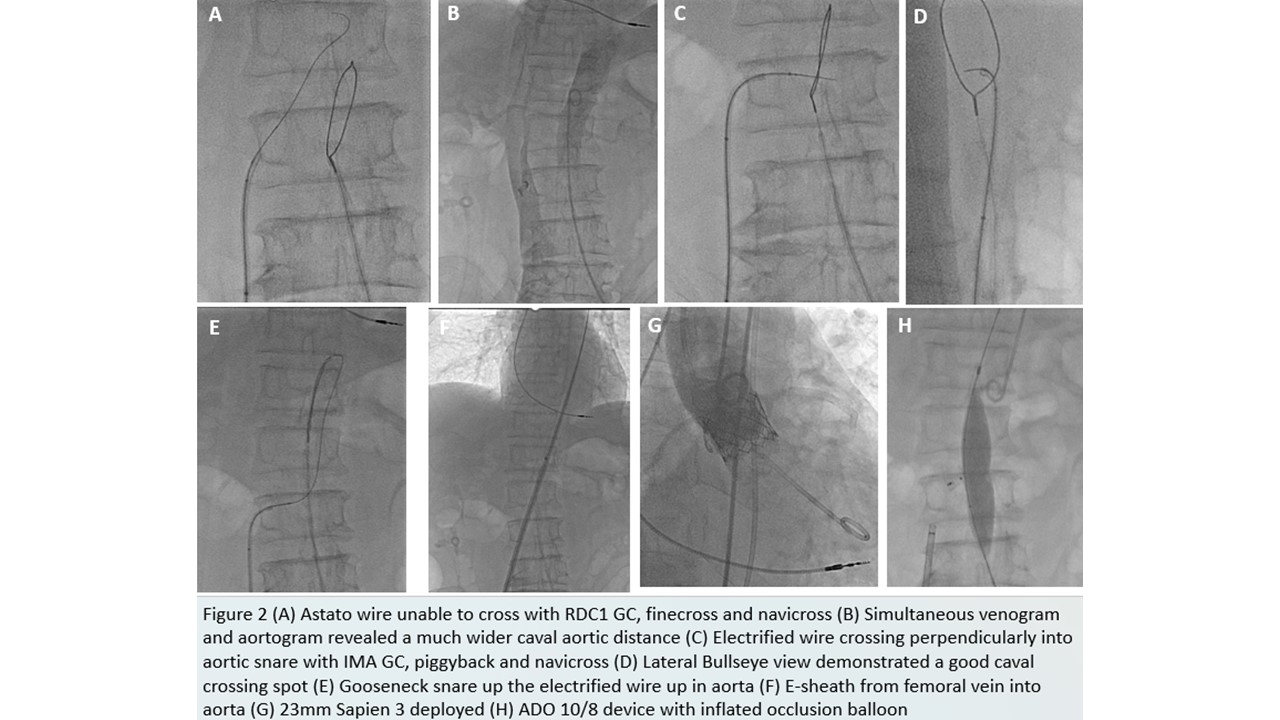
Under general anaesthesia, we performed percutaneous coronary intervention to LAD first. Then, we prepared for the transcaval crossing. Left femoral access was obtained and inserted the 25mm gooseneck snare position at the top of L3. Renal length RDC-1 guiding catheter (GC) was used from right femoral vein, with Astato XS 40 300cm wire over finecross microcatheter and Navicross (90cm). However, it was unsuccessful and hence exchanged to RDC renal length with piggyback MC and navicross. Despite that, electrified wire still could not cross the intended spot.
We performed a simultaneous venogram and aortogram together and revealed a significant wider caval-aortic distance compared to the preoperative CT. As this could be due to volume depletion, intravenous fluids were given. As the IVC diameter was smaller, the guiding catheter was exchanged to IMA, together with piggyback and navicross microcathter. This was successfully performed and able to deliver the lunderquist wire over with 14Fr E sheath inserted.
The TAVI was then performed and deployed a 23mm Sapien 3 valve according to preoperative CT annulus sizing.
Transcaval closure was performed using ADO 10/8 device and Atlas 18x40mm occlusion balloon was used. Final aortogram showed mild residual shunt only.
Case Summary
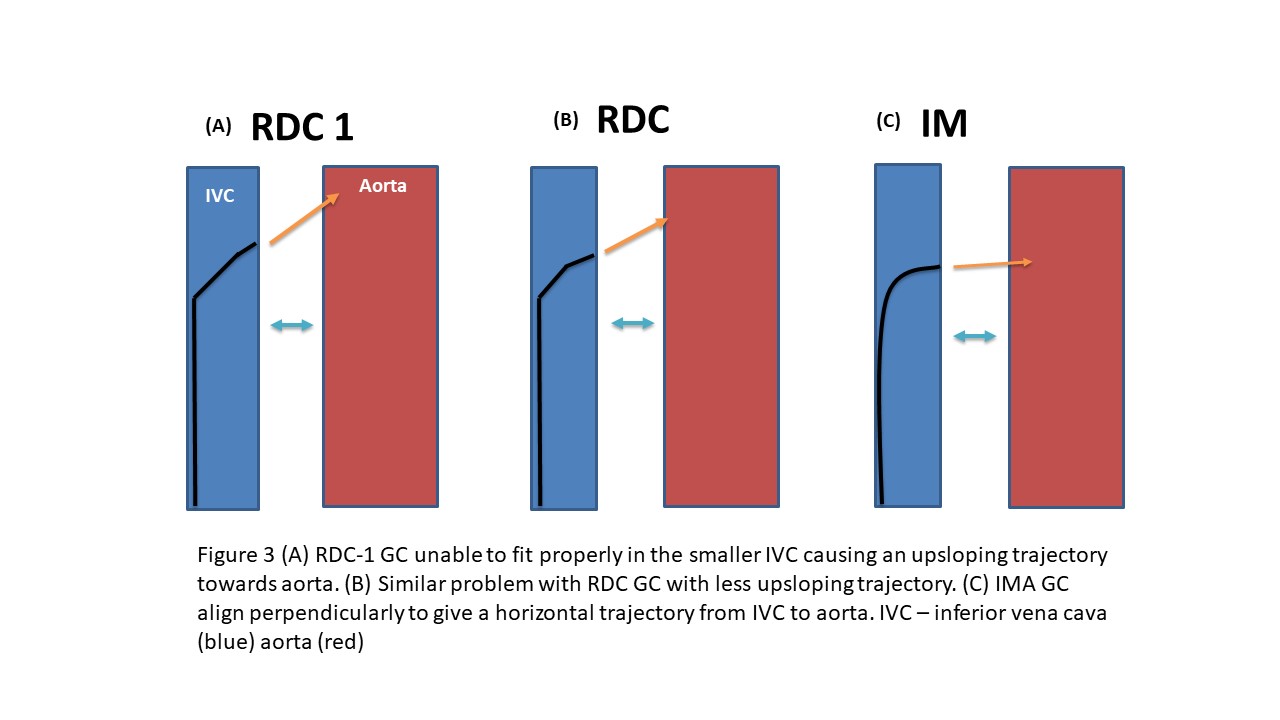
Caval-aortic distance could be wider due to the volume status of the patient. In view of a smaller IVC diameter, despite a stronger RDC1 support guiding catheter could deflect the trajectory of the wire crossing as the size of IVC could not fit the guiding catheter well. Switching to IMA catheter became an important step to align the angle of crossing well between IVC and aorta. So, guiding catheter support strength is not always the key. Although not routinely performed, a simultaneous venogram and aortogram could reveal a better vision and anticipate any difficulty for caval crossing. It would be important to tailor different anatomy accordingly to facilitate successful transcaval TAVI.