
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-039
Choices, Options, Decisions Abound. Choose Right, Take the Best Option and Decide Well.
By Iskandar Mirza Amran
Presenter
Iskandar Mirza Amran
Authors
Iskandar Mirza Amran1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-039
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Choices, Options, Decisions Abound. Choose Right, Take the Best Option and Decide Well.
Iskandar Mirza Amran1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
I.M Amran
Relevant Clinical History and Physical Exam
67 years old gentleman with known case of diabetes mellitus type 2, hypertension, dyslipidemia and obesity was referred to National Heart Institute (IJN) to rule out coronary artery disease in view of chest pain with exertion.
Relevant Test Results Prior to Catheterization
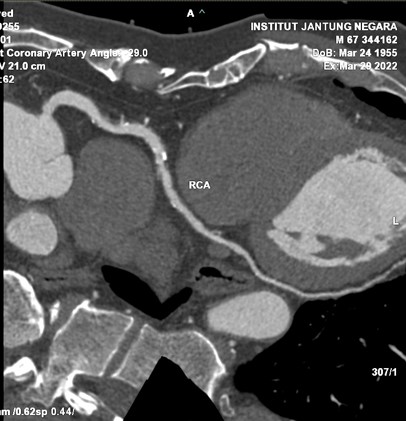
MSCT cardiac was done and showed calcium score of 1108 Agaston (LM-104, LAD-492, LCx-43, RCA-469) with moderate to severe mixed calcified atherosclerotic disease at the ostial-proximal and mid segments of the LAD, LCx and RCA segment.


Relevant Catheterization Findings
Left main stem: no stenosis
Interventional Management
Procedural Step
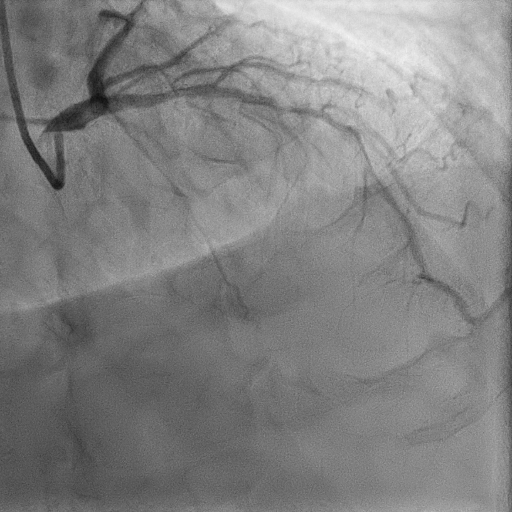
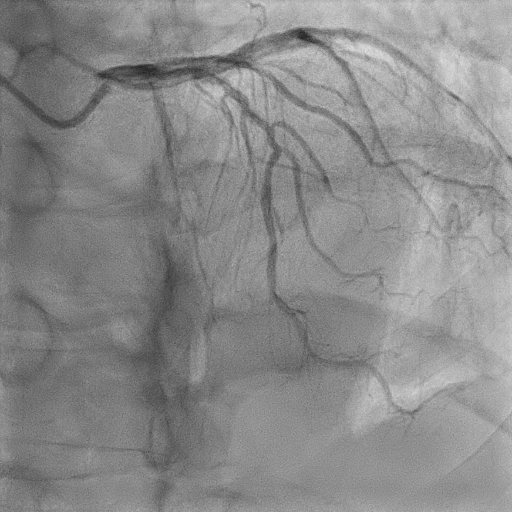
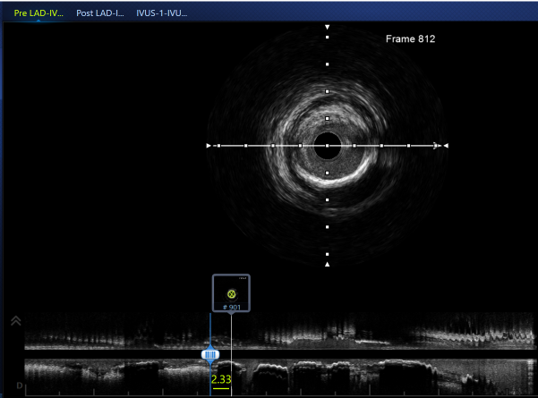
Diagnostic angiogram was done using optitorque, results as mentioned above. EBU 3.5 6 Fr is used. Run through floppy advanced to the lesion in left descending artery. Intravascular ultrasound (IVUS) is done to study the calcified lesion. IVUS showed 360-degree calcified ring lesion at proximal LAD region. However, length of calcification is only 3 mm. Thus, decided to use scoring balloon to prepare the lesion. Lesion was predilated using NC scoring balloon 2.5/15 mm and inflated up to 26 atm, however failed to crack the open the lesion. NC scoring balloon 3.0/15 mm was then used and dilated up to 26 atm, but we still failed to crack the calcium and noted to have minimal non-flow limiting dissection. Decided to use intravascular lithotripsy IVL C2 3.0/12 mm and instrument advanced to the lesion and shock wave delivered. At 8th shock wave. lesion was successfully opened. Lesion was then stented with 2 drug eluting stents,3.0/36 mm (at mid segment) and 3.5/24 mm (proximal LAD). Both stents was postdilate using NC 3.0/15 mm(distal stent) and NC 4.0/15 mm (proximal stent). Final IVUS showed an excellent minimal stent area with final shots showing good TIMI 3 flow.

Case Summary
Optimal plaque preparation of calcified coronary lesions is key to prevent stent failure. Percutaneous coronary intervention of heavily calcified stenoses remains significant challenge to interventional cardiologist. Current percutaneous coronary intervention strategies with high and ultra-high pressure dilatation, scoring/cutting balloons, and atherectomy are associated with a higher complication rate. IVL provide a valid strategy for lesion preparation in severely calcified coronary lesions with high success rate, low procedural complications and low major adverse cardiovascular event rates.