Angiographic Evaluation of a New Technique for Common Femoral Artery Access: The Inguinal Ligament-Guided
Beijing Anzhen Hospital, Capital Medical University, Beijing, China
S.P. Nie, E.P. LOPES LAO, C.Q. Jia, Y. Zhang, Q. Lv, X.M. Liu, J.H. Wu, Y. Qiao, J. Li, T.Y. Luo, J.Z. Dong, X.H. Liu, C.S. Ma
Background: Various techniques have been used to acquire common femoral artery (CFA) access which was associated with lower risk of complications in percutaneous catheterization. A relatively simple, safe and reliable technique was expected.
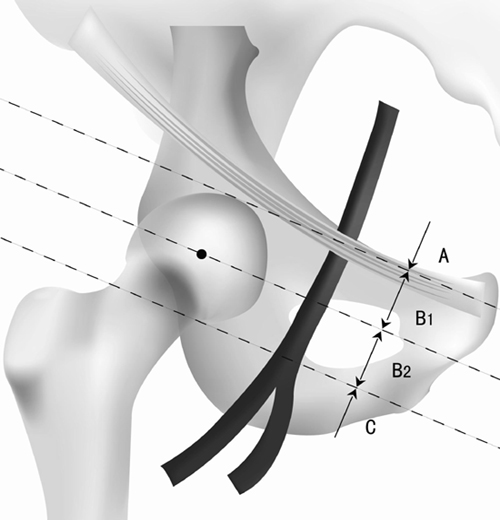
Methods: We introduced a new inguinal ligament-guided technique and inguinal division. Eight hundred and twenty-two unselected patients undergoing transfemoral percutaneous coronary catheterization from 2004 to 2009 were studied. After locating the inguinal ligament, a reference to conduct artery puncture site, medius pinpointed the intersection of inguinal ligament and femoral artery. Artery puncture was then performed at the inferior margin of forefinger. By femoral angiogram, we utilized femoral head as a landmark, of which the midpoint, inferior and superior margin were referred to borderlines, to divide inguinal region into zone A, B1, B2 and C for femoral artery cannulation. Femoral head (zone B) was defined as the optimal area of femoral artery puncture (Figure).
Results: Successful CFA cannulation occurred in 82.8% of cases. Arterial puncture over the femoral head (zone B) occurred in 96.8% (796/822) of patients, 36.0% (296/822) for zone B1 and 60.8% (500/822) for zone B2, respectively. When femoral artery puncture located on zone B, B1 B2 and C, CFA cannulation occurred in 83.9% (668/796), 91.6% (271/296), 79.4% (397/500) and 40% (8/20), respectively.
Conclusion: Inguinal ligament is a reliable reference for guiding the puncture of CFA in transfemoral percutaneous catheterization.